Overweight and obesity are determinant risk factors of chronic disease; they are considered as public health problems since they can promote diabetes mellitus, cardiovascular disease and cancer, which are among the most crippling non-communicable diseases. Currently, the epidemiological trend in most countries show that the cause of death is changing from infectious diseases to non-infectious diseases. According to statistics from the World Health Organization (WHO), non-communicable diseases are responsible for 63% of deaths worldwide, double the number of deaths from infectious diseases. 1 The World Health Assembly calls for the strategy to prevent and control non-communicable diseases by practicing a healthy lifestyle. People should eat a healthy diet, exercise to manage overweight and obesity.2
The prevalence of obesity increases in both developed and developing countries, whether in high or in low economic level. In the United States of America (USA), the prevalence of obesity in 1994 was 23%, and this rose to 31% by the year 2000.3
In Indonesia, the 2007 national data indicated an obesity prevalence of 19.1% among individuals aged15 years and older.4
Young people are dynamic and productive;5 and are expected to keep optimal health condition, so they can perform well in life. There is a strong correlation between obesity and degenerative diseases, this paper means to explore the determinant factors of overweight and obesity among young adults, and the related health condition that exist in these obese Indonesians. If the data indicate there are health problems among overweight and obese young adults, these can serve as early warning tools for all stakeholders to develop a system and management program of obesity prevention for younger age group.
This paper presents the result of national wide data analyses from 2007 basic health research (NIHRD, Ministry of Health). Data were collected cross-sectionally from 33 provinces, 440 sub-districts, which covered 973.662 samples from ages 1 to 97 years old. Samples were the sa me as the core of Susenas Kor (National Socioeconomic Survey Core) of urban and rural area of the Central Bureau of Statistics (277,630 households). Data were collected by trained local enumerators with at least a bachelor graduate degree. Data about socio-demographic factors andlifestyle were collected by interviewing subjects using questionnaires. Anthropometric data (weight, height, waist circumference) and blood pressure were measured by trained surveyors, height by microtoise, weight by digital scale, waist circumference by centimeter scale and blood pressure by using a digital tensimeter. Blood glucose data was obtained from 10% of the total subjects in urban area aged 15 years and older. After overnight fasting (10 -14 hours) all subjects except those who were previously diagnosed with diabetes mellitus (DM) were given an Oral Glucose Tolerance Test (OGTT). Solution of 75 g glucose in 200 ml water was given to the respondent, then a 2-hours postload, venous plasma glucose was measured using Chemical clinic automatic or using spectro-photometry measurement. 4
The data in this paper came from 80,254 female and 73,588 male subjects aged 19-29 years, who live in either a rural or urban area. The blood glucose data came from 2,386 female and 1,922 male subjects of the same age range, but only from urban areas.
Data were analyzed using SPSS 15 software for complex samples. Binary logistic regression was used to analyze the determinant variables. All subjects received both written and oral information about the purpose of the research, so they gave their consent to take part in the survey. The research protocol was approved by the Ethics Committee of the National Institute of Health Research and Development.
Overweight and obese were determined using the Asia-Pacific WHO criteria. Central obesity is waist circumference (WC) > 80 cm in women and > 90 cm in men. Hypertension was defined according to JNC-VII criteria or history of intake of anti hypertensive medicines. Diabetes Mellitus (DM) was defined as blood glucose level 200 mg/dl 2 hours after a glucose load. Impaired glucose tolerance (IGT) was defined as a glucose level between 140- < 200 mg/dl 2 hours after glucose load.6 Sufficient physical activity is defined as MET > 600 (WHO steps).Economic level was categorized into 5 quintiles based on the per capita expense (Survey sosial-ekonomi nasional/Susenas Data). Quintiles 1-2 was categorized as poor, quintiles 3-5 as not poor. Low education level is equivalent to junior high graduate, middle education level is equivalent to senior high graduate, and high education level is equivalent to college graduate. Unemployment is categorized as having no source of income, they may get money from donations.
Data in Table 1 indicate the prevalence of overweight as 13.0% (female 13.4% and male 12.6%). The prevalence of obesity was 11.8% (female 15.0% and male 8.3%). The prevalence of overweight or obese increased with age. Prevalence of obese is higher among females, married couples, and people living in urban setting. Housewives, officers, businessmen and highly educated people also have higher prevalence. Even though the trend of obesity rises with higher spending, the prevalence of overweight and obesity in people in lower economic levels is also high. There were 13.4% overweight and 12.4% obese in high socio-economic groups, and 12.2 % overweight and 10.9% obese in low socio-economic groups.
Click here to download Table 1
Table 1. Nutritional status of young adults based on subject characteristics
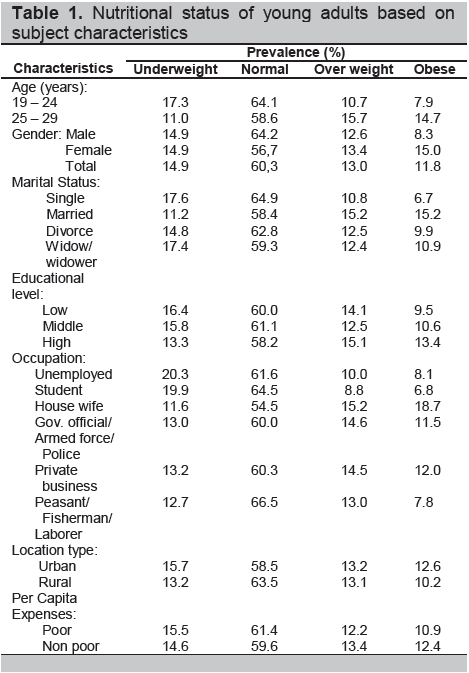
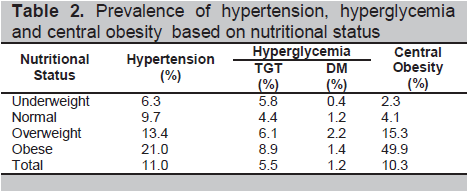
Table 2 shows that the prevalence of degenerative diseases such hypertension and hyperglycemia are higher in overweight and obese than in other groups. Hypertension was prevalent in 13.4% of overweight and 21.0% of obese, in comparison to 9.7% among normal subjects. The prevalence of IGT and diabetes mellitus were 6.1% and 2.2% among overweight; 8.9% and 1.4% among obese subjects, respectively. Central obesity is present in 15.3% of overweight and 49.9% of obese subjects. Table 3 shows that overweight and obese persons had 1.8 times the risk of hypertension (95% CI 1.7 – 1.9. p= 0.0001) compared to normal body mass index (BMI), while the risk for IGT and DM are 1.8 times higher (CI 1.4 – 2.3. p= 0.0001) and the risk for central obesity was 10.5 times (CI 10.0 – 11.1. p= 0001).
Click here to download Table2
Table 2. Prevalence of hypertension, hyperglycemia and central obesity based on nutritional status
Click here to download Table 3
Table 3 . Bivariate association between overweight and obesity with hypertension, IGT, DM, and central obesity
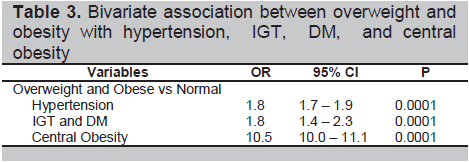
Table 4 shows that 25-29-year old subjects had 1.82 times the risk of overweight and obesity (CI 1.77 – 1.88. p= 0.0001) compared to 18 – 24 year – old subjects.
Click here to download Table 4
Table 4. Bivariate association between characteristic of socio-demography, lifestyle with overweight and obesity
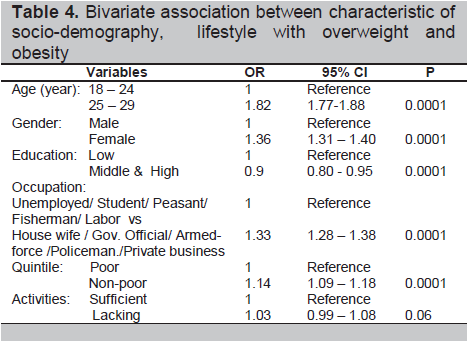
Females have higher relative risk at 1.36 to be overweight and obese, compared to male subjects. Middle and high education had 0.9 the risk to be overweight and obese compared to low education groups.House wives, government officials, armed forces staff, policemen, and private entrepreneurs have 1.33 times risk to become overweight and obese. People in higher socio-economic status have 1.14 times higher risk to be overweight and obese compared to poor people.
Lack of activity had no significant effect on outcomes measured compared with sufficient activity (p= 0.06). The effect of eating fruits and vegetables ≥ 5 portions/day could not be analyzed due to the limited data available.
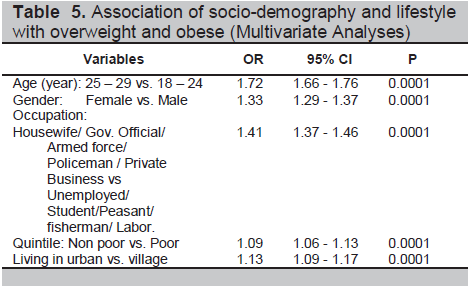
Table 5 shows the result of multivariate analyses, in which the determining factor for overweight and obesity was older age. The group aged 25 – 29 years had 1.72 times (95% CI 1.66-1.76, p 0.0001) higher risk to be overweight and obese compared to the group aged 18 – 24 years.. Based on gender, females had higher risk to be overweight and obese, which is 1.33 times higher (CI 1.29 – 1.37, p 0.0001) than males. Housewives, government officials, military personnel, policemen, private entrepreneurs are 1.41 times (CI 1.37-1.46, p 0.0001) more likely to be overweight and obese than the unemployed subjects, students, peasants, fishermen, laborers. Urban people are 1.13 (CI: 1.09 -1.17, P 0.0001) times more likely to be overweight and obese than rural villagers, and the affluent group has 1.09 times (CI: 1.06 -1.13, p 0.0001) higher risk than poor people.
Click here to download Table 5
Table 5 . Association of socio-demography and lifestyle with overweight and obese (Multivariate Analyses)
The prevalence of overweight and obesity in young adults is high in Indonesia, and this could be related to childhood obesity. Obesity during childhood tends to continue until adulthood.7 Prevalence of overweight and obesity at age 6–14 years old in Indonesia was 9.5% in male and 6.4% in female. Management of overweight and obesity has to start earlier in this age group. Since the prevalence increased by age, this suggests that age is a determinant factor in the development of obesity. The same observation is happening in the USA and other countries, the older age group tends to be obese ; and this may be caused by low energy expenditure due to decreased basal metabolic rate with increasing age.8 The prevalence of overweight and obesity for young males was 12.6 % and 8.3%, prevalence for young females was even higher, which was 13.4% and 15.0%. Prevalence of overweight and obesity on the national level was 13.9 % for males and 23.8% for females. This may be affected by the wide range of age, which is 15 – 97 years old.4 In 2002, prevalence of obesity (BMI ≥30) of Americans age ≥ 18 years old was 22.3 % in male and 20.4% in female; in 2004 the prevalence became 23.8% in male and 21.7% in female.3 Both data sets indicate that obesity prevalence is lower in females than in males. In 1993, obesity prevalence among British males age ≥ 19 years old was 13.6 % and it rose to 24% in 2004; while in females, it was 16.9% and increased to 24.4%.9 The different prevalence of overweight and obesity based on gender may be caused by many factors, including food habits and lifestyle. There might be similar factors causing more obesity among British and Indonesian females compared to their male counterparts. Some studies agreed that the higher the economic status, the higher the prevalence of obesity; this study reported that poor communities had higher overweight (12.2%) and obesity (10.9%) prevalence. The burden of obesity is shifting towards the poor.10,11 Obesity is higher among urban dwellers. Ziraba found out that overweight and obesity in urban areas become health problems among both the rich or the poor populations. Living in urban areas is related to reduced opportunities to engage in physical activity. These problems call for preventive action in all levels of the population. Surveillance and prevention strategies to fight overweight and obesity should be improved to address the increase in prevalence.
Hypertension prevalence in overweight and obese people is 1.8 times higher than people with normal BMI. Impaired glucose tolerance and DM incidence are 1.8 times higher than normal BMI. The higher the overweight and obesity incidence, the higher the prevalence of hypertension and hyperglycemia. Macmohan et al. reported that hypertension rise linearly with body weight or BMI.14
Overweight and obese people have 10.5 times the likelihood to have central obesity than people with normal BMI. Central obesity has strong association with some chronic disease risks. Studies indicate that the increase in BMI and central obesity correlate with mortality risk.15 Some other studies indicate that obesity in young adult male is a strong risk factor for cardiovascular disease, regardless of the body fat distribution.16 Steinberger et al. found that obesity and insulin resistance are also cardiovascular risk factors, and by lowering body weight or BMI by 5-10% type 2 diabetes can be prevented.17
Lack of physical activity in this study had no statistically significant effect (p= 0.06) on overweight and obese status, maybe the overweight & obese group had increased activity in an effort to slim down.
The subgroup of housewives had highest risk to be obese. Navade et al. found out that housewives had higher risk to be obese than employed women. 18 Health care programs have to be developed to reduce obesity in this group.
The prevalence of overweight and obesity in young adults in Indonesia is 13.0% and 11.8%, respectively. The prevalence is higher in females than in males. The prevalence is already high in low socio-economic population, and becoming higher with the increase in economic status. Prevalence of hypertension and hyperglycemia are higher in overweight and obese people than in normal body mass index population.
Since obesity prevails in all economic levels, it is important to determine the real cause of obesity in Indonesian young adults. There is a need to collect data on individual food consumption, so that we can discover the type of nutrient imbalance in these groups. The type of local foods may also affect the incidence of obesity in each province in Indonesia; and the physical activity habits in each province with different cultures may also have important roles.
Considering the high prevalence of overweight and obesity in young adults, followed by the increase in hypertension and hyperglycemia incidences, a national strategy on diet, physical activity and health care has to be developed to prevent overweight and obesity at an earlier age.
Our gratitude is extended to Dr. d Trihono, Director of NIHRD; Prof./ Dr. Agus Purwadianto SH. MSi. SPF(K) and Dr Triono Soendoro, PhD as former directors of NIHRD and as the Basic Health Research (BHR) designer; Dr. Endang Sedyaningsih, MPH,DrPH. The active Minister of Health, and Drs. Ondri Dwi Sampurno Msi. Apt. the Head of Center for Biomedical and Basic Technology for Health, for their support and approval to use 2007 BHR data to be analyzed.
We highly appreciate all the help and hard work of the Data Management team and the BHR Secretariat, in providing us with the important data needed. Endless thanks to Scientific Board, surveyors, laboratory technicians, respondents, and related team in all provincies. May God bless us.
1. The Surf report: Surveillance of risk factors related to noncommunicable diseases: Current status of global data. Geneva (CH): World Health Organization, 2003.
2. World Health Organization. Prevention and control of noncommunicable diseases: Implementation of the global strategy. 63rd World Health Assembly. 1 April 2010; 2- 6.
3. Van Wye G, Kerker BD, Matte T, Chamany S, Eisenhower D, et al. Obesity and Diabetes in New York City. 2002 and 2004. Prev Chronic Dis, April, 2008; 5(2): A48.
4. National Institute Health Research and Development. Riskesdas report. Jakarta: 2007, pp 48– 53.
5. Lester A. Lefton. Psychology. Boston: Allyn and Bacon Viacom Company: 1997; p. 368
6. WHO. Definition and diagnosis of diabetes mellitus and intermediate hyperglycaemia. Geneva: WHO: 2006; pp. 9-43
7. Serdula MK., Ivery D, Coates RJ , Freedman DS , et al. Do obese children become obese adults? Preventive Medicine.1993; 22(2): 167 - 177
8. Harris J, Benedict F . A Biometric Study of Human Basal Metabolism. PNAS 1918; 4 (12): 370–3.
9. Zaninotto P. Head J. Stamatakis E. Wardle H. Mindell J. Trends in obesity among adults in England from 1993 to 2004 by age and social class and projections of prevalence to 2012. J Epidemiol Community Health, 2008; 0 :1–7.
10. Popkin BM and Larsen PG. The nutrition transition: Worldwide obesity dynamics and their determinants. International Journal of Obesity 2004; 28: S2–S9.
11. Deborah B, Nicolas F. Developing comprehensive approaches to prevention and control of obesity among low-income, urban, African-American women. Journal of the American Women’s Association 2001; 56: 59-64.
12. Ziraba AK, Fotso JC. Overweight and obesity in urban Africa: A problem of the rich or the poor? BMC Public Health 2009; 9:465
13. The challenge of obesity in the WHO European Region and the strategies for Response. Copenhagen, WHO Regional Office for Europe, 2007
14. Macmohan S, Cutter J, Britain E, Higgins M. Obesity and hypertension: epidemiological and clinical issues. Eur Heart J 1987; 8 (suppl B): 57-70.
15. Pischon T., Boeing H., Hoffmann K., Bergmann M., et al. General and abdominal adiposity and risk of death in Europe. The New England Journal of Medicine 2008; 359 (20): 2105 - 2120
16. Australian Institute of Health and Welfare and National Heart Foundation of Australia. The relationship between overweight, obesity and cardiovascular disease. Australian Institute of Health and Welfare. Canberra, 2004.
17. Steinberger J., Moran A., Prineas RJ., Vessby B. et al. Obesity and insulin resistance fuels cardiovascular risk factors in teens. Circulation 2005; (23): 22 – 23.
18. Navadeh S., Sajadi L., Mirzazadeh A., Asgari F., Haghazali M. Housewives' obesity determinant factors in Iran; National survey – stepwise approach to surveillance. Irainian Journal of Public Health 2011; 40(2): 87 – 95.
Articles and any other material published in the JAFES represent the work of the author(s) and should not be construed to reflect the opinions of the Editors or the Publisher.
Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.