Subacute thyroiditis, also called de Quervain's thyroiditis, is the most common cause of thyroidal pain. Symptoms and signs of subacute thyroiditis include a prodrome of myalgia, pharyngitis, low-grade fever and fatigue, followed by a tender, diffuse goiter and neck pain that often radiates to the ear.1,2 A variety of viruses have been implicated as the cause of SAT, including those that cause mumps, measles, primary human immunodeficiency virus infection and influenza.3 However, it is regarded as a relatively rare condition as few patients who develop a viral infection ever have thyroiditis. In the early phase of SAT, which usually lasts 3 to 6 weeks, about 50% of patients have an initial thyrotoxic phase due to release of preformed thyroid hormone. About one-third of patients subsequently enter a transient hypothyroid phase that can last up to 6 months.2 Because permanent hypothyroidism has been reported in 10 to 15 percent of patients, close follow-up after resolution of the early phase is essential.4
There is considerable variation in the mode of onset and the severity of SAT. Outbreaks of SAT have been described in reports from Japan and Italy, with highest rates coincident with peak infection rates of echovirus and coxsackie virus groups A and B during summer months.5,6 In recent years, the number of SAT patients in our clinical practices seems to have markedly increased. Because of this observation, we sought to characterize the clinical presentation and outcomes in Thai patients with SAT.
We conducted a review of records of all SAT patients who were treated in Theptarin Hospital, Bangkok, Thailand from January 2007 to December 2013. The diagnosis of SAT was based on clinical features of pain and tenderness in the region of the thyroid gland over one or both lobes, laboratory findings of elevated erythrocyte sedimentation rate (ESR) or elevated C-reactive protein (CRP), elevated serum free thyroxine (FT4) and decreased serum thyroid stimulating hormone (TSH), or suppressed 24-hour radioactive iodine uptake (RAIU). Total triiodothyronine (TT3), FT4, TSH, thyroglobulin autoantibodies (anti-Tg) and thyroid peroxidase antibodies (anti-TPO) were measured using electrochemiluminescent immunoassays (Roche Diagnostics, Indianapolis, USA). The onset of subacute thyroiditis was defined as the date at which patients first experienced of thyroid pain. Patients who were lost to follow-up before completion of treatment were excluded from this study. Clinical characteristics, laboratory findings, modes of treatment, and complications were noted. This retrospective study was approved by the Ethical Board Committee of the Theptarin Hospital.
Statistical AnalysisContinuous variables were summarized as mean ± standard deviation (SD), while categorical variables were described in a frequency table. Characteristics of patients who developed and did not develop permanent hypothyroidism was compared using unpaired t-test for continuous variables and Chi-square test for categorical variables. The level of significance was set at 0.05. All statistical analyses were conducted using the Statistical Package for the Social Sciences version 17.0 (SPSS, Illinois, USA).
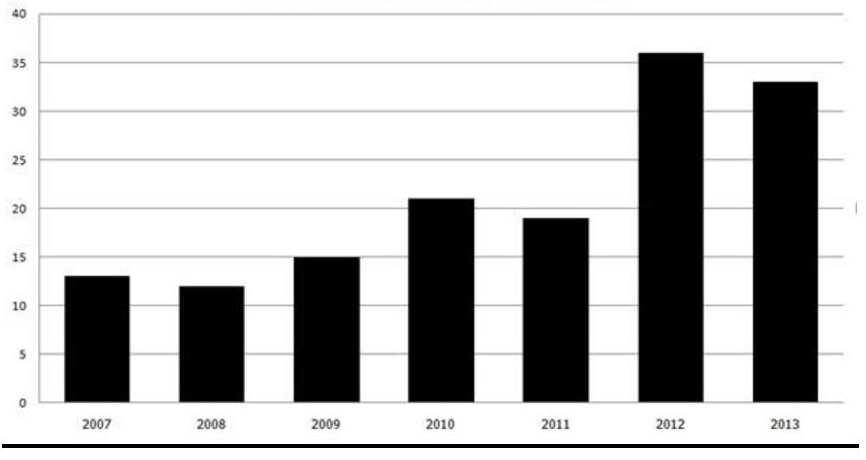
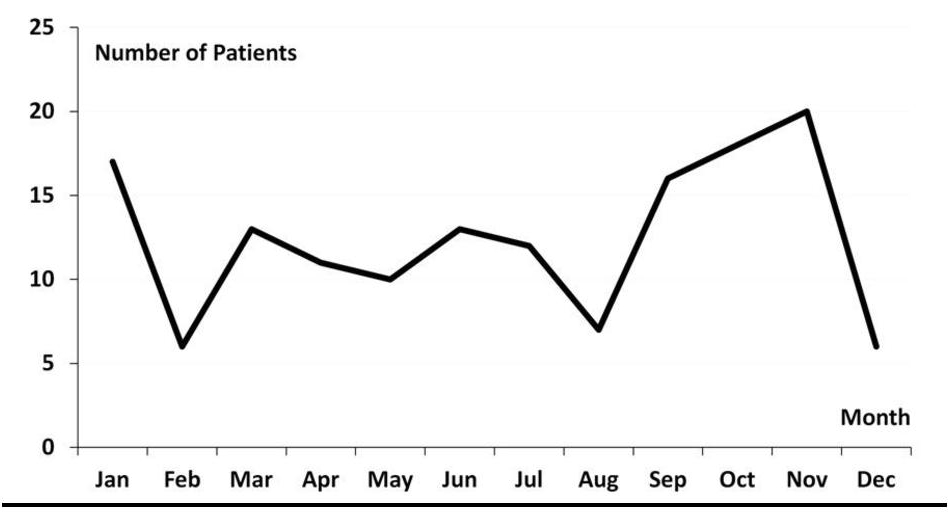
From January 2007 to December 2013, subacute thyroiditis was diagnosed in 149 patients, with peak occurrence in October and November (32.2%) (Figure 1). Only 115 patients had complete follow-up data. In these patients, the mean age was 43.8 ± 10.8 years and 88.7% were women. An upper respiratory tract infection preceded SAT in 68.7% of cases. At the onset of SAT, 45.0% of patients experienced unilateral neck pain. 47.0% of patients had temperature readings greater than 38°C. Typical symptoms associated with thyrotoxicosis, including palpitations, increased sweating and weight loss, were reported by 67.1% of patients. On the first visit, thyroid nodules were apparent on physical examination in 29 patients (25.2%), but only 3 of these patients continued to have thyroid nodules after the resolution of SAT. Subsequent fine needle aspiration cytology in these patients revealed benign colloidal nodules.
Click here to download Figure 1Figure 1. Frequency distribution of subacute thyroiditis patients by year, 2007-2013.
Click here to download Figure 2
Figure 2. Frequency distribution of subacute thyroiditis in Thai patients by month, 2007-2013.
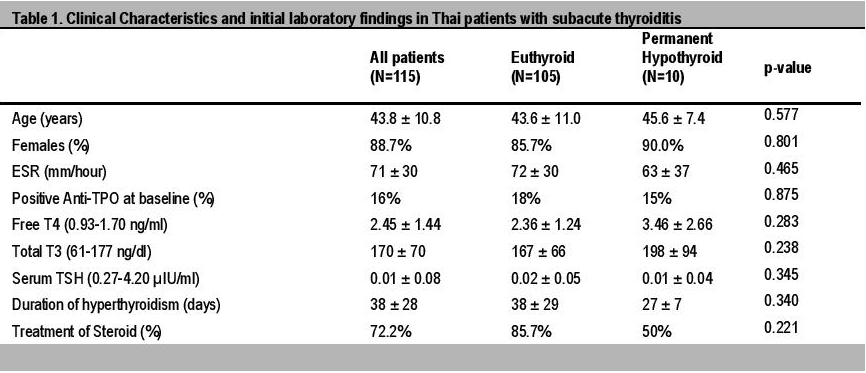
Anti-TPO levels measured in 69 patients showed positive results in 16% of cases (median titer 382 IU/mL). Positive anti-Tg levels were also seen in 36% of the 83 patients with this test (median titer 280 IU/mL). Clinical characteristics and initial laboratory findings are summarized in Table 1.
Click here to download Table 1Table 1. Clinical characteristics and initial laboratory findings in Thai patients with subacute thyroiditis.
A 24-hour RAIU was done in 7 patients with uncertain diagnosis. All 7 showed very low uptake of less than 5%. Thyroid ultrasonography done in 25 patients showed mild thyroid enlargement with homogeneous echotexture and hypoechoic areas consistent with inflammation. Fine-needle aspiration biopsy of the thyroid (FNA) was done in 4 patients with uncertain diagnosis on initial visit. Results showed multinucleated giant cells with thick colloid, typical cytologic results for subacute thyroiditis.
Among 115 patients, 83 (72.2%) received monotherapy with prednisolone at an initial dose of 10 to 60 mg/day, with a median of 30 mg/day. Nonsteroidal anti-inflammatory drugs (NSAIDs) or cyclooxygenase-2 (COX-2) inhibitors were given to 25 patients (21.7%), while 7 (6.1%) were observed without any treatment. For the group receiving NSAIDs or COX-2 inhibitors, etoricoxib 90 to 120 mg/day was the most commonly used, followed by ibuprofen 800 to 1,200 mg/day in divided doses. The mean length of time for complete alleviation of pain was 5 days for the successful NSAIDs group (15 patients). The remaining 10 patients who received NSAIDs required prednisolone as rescue treatment. In the group that received prednisolone as initial treatment, continuation and tapering of medication lasted for a median duration of 49 days (range 6 to 194 days). Recurrence of SAT during the tapering period was observed in 14 patients, and late recurrence of SAT necessitated the need to restart steroids in 15 patients. Steroid side effects, such as acne, oily skin, irritability were tolerated well by most patients. One diabetic patient needed to stop steroid treatment because of worsening glycemic control. The steroid-treated patients gained 2 kg on the average during the course of treatment.
Throughout the specified review period, recurrent episodes of SAT after treatment accounted for 7.0% of all cases, with a median interim period of 5.5 years (range 1 to 20 years) between the first and second episodes. Transient and permanent hypothyroidism developed in 6.1% and 8.7% of patients respectively. Interestingly, overt autoimmune thyroid disease occurred following SAT in 3 cases. One case of Graves' disease occurred 2 months after the onset of SAT. There were 2 cases of Hashimoto's thyroiditis following SAT at 2 and 3 months. Unfortunately, baseline thyroid antibody levels were not available in these patients.
Subacute thyroiditis is an uncommon inflammatory disease of the thyroid gland which is usually self-limited. The pain typically radiates to the angle of jaw and to the ear on the affected side. Following initial unilateral pain, it may then progress to involve the contralateral side, a phenomenon called "creeping thyroiditis." Tenderness on palpation of the thyroid gland helps differentiate this condition from pharyngitis, a common misdiagnosis during the early stages.7 The peak incidences of SAT have been reported mostly during the summer and early autumn in regions with four seasons, including North America, Europe and Japan.5,8 We observed the occurrence of SAT peaked during October and November in Thailand. The significant seasonal cluster and increasing numbers of SAT cases in our clinic is coincides with the increasing rates of influenza observed in recent years in Thailand which demonstrated increased influenza rate from July to September (accounted for one third of annual influenza infection rate). Pandemic of Influenza subtype H1N1 emerged (60.65 of total positive samples) in mid-2009 and persisted in 2010 (53.35 of total positive samples).9
It is important to differentiate subacute thyroiditis from other causes of thyroidal pain, particularly acute suppurative thyroiditis, because steroid treatment would be catastrophic in bacterial infections. Acute suppurative thyroiditis is most often caused by gram-positive bacteria in the thyroid gland. Most patients have a preexisting thyroid disorder, typically nodular disease. Accompanying signs usually include infection in structures adjacent to the thyroid, local lymphadenopathy and fever. Chills may also be present if bacteremia occurs. Leucocytosis is seen in acute suppurative thyroiditis, in contrast to a usually normal white blood cell count in SAT. Symptoms are generally more obvious in acute suppurative thyroiditis than SAT.1
Other conditions which could mimic symptoms of SAT are hemorrhagic nodules or cysts, painful Hashimoto's thyroiditis, and rare cases of anaplastic thyroid cancer.2 In our study, the diagnosis of SAT was mostly based on typical clinical features and elevated ESR or CRP. The use of RAIU was only in more difficult cases that presented with thyrotoxicosis needing distinction from Graves' disease. Consistent with a previous study, thyroid nodules observed during the clinical course of SAT resolved spontaneously with resolution of inflammation.10 SAT may be distinguished from Graves' disease by the relatively smaller increase in triiodothyronine (T3) compared with thyroxine (T4) hormone concentrations. This change reflects T4 elevation from destructive thyroiditis and possibly from impairment of peripheral deiodination of T4 to T3 during acute illness. In previous studies, the total T3 to T4 ratio (calculated as ng/dL divided by μg/dL) is usually less than 20 in SAT, and the ratio of free T3 to free T4 is less than 4.3 in Thai patients.11,12 While this may aid in supporting the diagnosis of SAT, our study used mostly TT3 and FT4, so that this ratio could not be verified. In general, thyroid antibodies such as anti-Tg, anti-TPO and TSH-receptor antibodies are usually absent in patients with SAT. However, transient low titers of antibodies (mainly anti-Tg) may be found during the initial phase.4
Treatment is directed primarily at symptomatic relief of thyroidal pain and tenderness. Symptoms of hyperthyroidism also could be treated with beta-blockers such as propranolol or atenolol, until the FT4 concentration returns to normal.2
The American Thyroid Association (ATA) recommends NSAIDs as the initial treatment for SAT. Prednisone may be given at 40 to 60 mg daily, with tapering over 4 to 6 weeks, should NSAIDs fail to provide pain relief.13 Despite the reluctance of most physicians to use corticosteroids for this usually self-limited disorder, the response is often more rapid and dramatic compared to NSAIDs. Complete alleviation of pain is usually achieved within 24 hours after initiation, compared to several weeks on NSAIDs.14 In our experience, the use of glucocorticoids has proven to be invaluable in the treatment of a vast majority of patients, most of whom presented with relatively severe symptoms.
In previous studies, steroid treatment did not prevent early- or late-onset thyroid dysfunction after SAT.4,15 A recurrence of symptoms occurred in about 20% of patients during steroid tapering.15 We also found a high rate of recurrence of symptoms during the course of steroid tapering in our study. Careful monitoring and tapering of steroid is warranted in order to avoid prolonged steroid exposure.
Recently, a prospective study from Japan reported that oral prednisolone at an initial dose of 15 mg/day given as the first line treatment in SAT was effective in ameliorating symptoms in 80% of patients within 8 weeks.16 This interesting finding challenges our current concepts in the treatment of SAT as recommended by the ATA. Further studies should be done to confirm this finding.
SAT generally resolves completely in more than 90 to 95% of patients. However, transient hypothyroidism may occur and may persist for several weeks or months in severe cases.17 While permanent hypothyroidism is uncommon, it has been reported to occur in 5 to 15% even many years after the diagnosis.3 In our study population, we found a similar rate of permanent hypothyroidism in less than 10% of patients. The recurrence of SAT is rare, but may happen several years after resolution of the first episode.18 Familial occurrence of SAT with HLA-B35 has been reported, suggesting that SAT may occur in genetically predisposed individuals.19 Further studies on patients who develop multiple episodes of SAT may clarify the role of genetics in these exceptional cases.
Another noteworthy finding in our study is the appearance of overt autoimmune thyroid disease (AITD) following SAT in 3 patients within 3 months. It is very rare for SAT to progress to either Graves' disease or Hashimoto's thyroiditis. In previous case reports, most patients had negative baseline thyroid antibodies, so that the autoimmune process was postulated to have been triggered by the release of antigenic material from the inflamed thyroid gland.20,21
Subacute thyroiditis in our group of Thai patients showed a trend for seasonal clustering during the months of October and November, with considerable variation in the severity of disease. Oral prednisolone provided dramatic improvement of pain, but the recurrence of SAT was common in the course of steroid treatment. The development of AITD following SAT was seen to occur in some patients after the resolution of SAT. These findings emphasize the need for careful follow-up during steroid treatment and long-term surveillance for thyroid dysfunction.
Conflict of InterestThe authors declare that they have no conflict of interest.
1. Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003;348(26): 2646-55. http://dx.doi.org/10.1056/NEJMra021194.
2. Bindra A, Braunstein GD. Thyroiditis. Am Fam Physician. 2006;73(10):1769-76. 3. Samuels MH. Subacute, silent, and postpartum thyroiditis. Med Clin North Am 2012;96(2):223-33. 4. Fatourechi V, Aniszewski JP, Fatourechi GZ, et al. Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmstead County, Minnesota, study. J Clin Endocrinol Metab. 2003;88(5):2100-5. http://dx.doi.org/10.1210/jc.2002-021799. 5. Nishihara E, Ohye H, Amino N, et al. Clinical characteristics of 852 patients with subacute thyroiditis before treatment. Intern Med. 2008;47(8):725-9. http://dx.doi.org/10.2169/internalmedicine.47.0740. 6. Martino E, Buratti L, Bartalena L, et al. High prevalence of subacute thyroiditis during summer season in Italy. J Endocrinol Invest. 1987;10(3):321-3. http://dx.doi.org/10.1007/BF03348138. 7. Volpé R, Johnston MW. Subacute thyroiditis: A disease commonly mistaken for pharyngitis. Can Med Assoc J. 1957;77(4):297-307. 8. Erdem N, Erdogan M, Ozbek M et al. Demographic and clinical features of patients with subacute thyroiditis: Results of 169 patients from a single university center in Turkey. J Endocrinol Invest. 2007;30(7):546-50. http://dx.doi.org/10.1007/BF03346347. 9. Chittaganpitch M, Supawat K, Olsen SJ, et al. Influenza viruses in Thailand: 7 years of sentinel surveillance data, 2004-2010. Influenza Other Respir Viruses. 2012;6(4): 276-83. http://dx.doi.org/10.1111/j.1750-2659.2011.00302.x. 10. Hardoff R, Baron E, Sheinfeld M, et al. Localized manifestations of subacute thyroiditis presenting as solitary transient cold thyroid nodules. A report of 11 patients. Clin Nucl Med. 1995;20(11):981-4. 11. Amino N, Yabu Y, Miki T, et al. Serum ratio of triiodothyronine to thyroxine, and thyroxine-binding globulin and calcitonin concentrations in Graves' disease and destruction- induced thyrotoxicosis. J Clin Endocrinol Metab. 1981;53(1):113-6. http://dx.doi.org/10.1210/jcem-53-1-113. 12. Bhasipol A, Sriphrapradang C. Patterns of thyroid hormones in patients with newly diagnosed thyrotoxicosis. Poster session presented at the 30th Annual Meeting of the Royal College of Physicians of Thailand, 2014 April 23-26, Pattaya, Thailand. 13. Bahn Chair RS, Burch HB, Cooper DS, et al. Hyperthyroidism and other causes of thyrotoxicosis: Management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid. 2011;21(6):593-646. http://dx.doi.org/10.1089/thy.2010.0417. 14. Volpé R. The management of subacute (DeQuervain's) thyroiditis. Thyroid. 1993;3(3):253-5. http://dx.doi.org/10.1089/thy.1993.3.253. 15. Mizukoshi T, Noguchi S, Murakami T, et al. Evaluation of recurrence in 36 subacute thyroiditis patients managed with prednisolone. Intern Med. 2001;40(4):292-5. http://dx.doi.org/10.2169/internalmedicine.40.292. 16. Kubota S, Nishihara E, Kudo T, et al. Initial treatment with 15 mg of prednisolone daily is sufficient for most patients with subacute thyroiditis in Japan. Thyroid. 2013; 23(3):269-72. http://dx.doi.org/10.1089/thy.2012.0459. 17. Lio S, Pontecorvi A, Caruso M, et al. Transitory subclinical and permanent hypothyroidism in the course of subacute thyroiditis (de Quervain). Acta Endocrinol (Copenh). 1984;106(1):67-70. http://dx.doi.org/10.1530/acta.0.1060067. 18. Iitaka M, Momotani N, Ishii J, et al. Incidence of subacute thyroiditis recurrences after a prolonged latency: 24-year survey. J Clin Endocrinol Metab. 1996;81(2):466-9. http://dx.doi.org/10.1210/jcem.81.2.863251. 19. Kramer AB, Roozendaal C, Dullaart RP. Familial occurrence of subacute thyroiditis associated with human leukocyte antigen-B35.Thyroid. 2004;14(7):544-7. http://dx.doi.org/10.1089/1050725041517048. 20. Wartofsky L, Schaaf M. Graves' disease with thyrotoxicosis following subacute thyroiditis. Am J Med. 1987;83(4):761-4. http://dx.doi.org/10.1016/0002-9343(87)90910-7. 21. Fukata S, Matsuzuka F, Kobayashi A, et al. Development of Graves' disease after subacute thyroiditis: two unusual cases. Acta Endocrinol (Copenh). 1992;126(6):495-6. http://dx.doi.org/10.1530/acta.0.1260495. 22. Minciullo PL, Ruggeri RM, Vita G, et al. Development of Hashimoto's thyroiditis after subacute thyroiditis: An unusual patient. Thyroid. 2009;19(1):734. http://dx.doi.org/10.1089/thy.2008.0234.Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.