Polycystic ovary syndrome (PCOS) was first reported by Stein and Levanthal in 1935 and is one of the most common reproductive endocrinopathies affecting about 8-11% of women in the reproductive age group diagnosed according to National Institute of Health (NIH),1-2 and probably up to 15-20% according to the Rotterdam consensus criteria. Despite being heterogeneous in nature, its cardinal features are hyperandrogenism, the presence of typical ultrasound features of polycyctic ovaries and chronic anovulation.3
The causes of PCOS are unknown,4 however insulin resistance is often increased in women with PCOS and hyperinsulinemia is an important feature of this condition, although neither is mandatory for the diagnosis.3 Insulin resistance in women with PCOS appears both in obese and non-obese women.5,6 There is increasing evidence that PCOS has implications for adverse pregnancy outcomes. Studies suggest that pregnancies in PCOS patients are characterized by more frequent complications, including early pregnancy loss, gestational diabetes, pregnancy-induced hypertension, preterm births and neonatal admission to intensive care units.7,8
With the high prevalence of complications in PCOS and its significant impact on patients' health, much has been done to evaluate the effects of insulin sensitizers in this regard. Metformin, an insulin-sensitizing drug, is perhaps the most widely studied agent and most, but not all uncontrolled studies have shown a significant improvement in insulin sensitivity. Metformin is currently utilized to treat PCOS patients with the aim of improving their metabolic, endocrine and ovulatory derangements. 7
Metformin (1.5-2.55g/day) ameliorates the endocrinopathy of PCOS by reducing fasting insulin, decreasing luteinizing hormone (LH) and androgen levels 9 with a return of regular menstrual cycles and ovulation in 55% 10 to 91% 11 of adult women and 91% of teenage girls. 12
Once their normal periods resume, these women are capable of becoming pregnant. Once they are pregnant, the question is whether metformin should be continued in an attempt to reduce the incidence of gestational diabetes, pregnancy-induced hypertension, preterm births and early pregnancy loss.
Of the commercially available oral hypoglycemic agents, only metformin has a reassuring safety profile for use in pregnancy.8,13 Metformin is classified a category B drug during pregnancy according to the United States Food and Drug Administration (USFDA), which means that metformin has no known fetal teratogenicity, although it crosses the placenta.14 Metformin has been used in the treatment of type 2 diabetes mellitus (T2DM) in pregnant women with no increase in the incidence of major congenital anomalies when compared with untreated pregnant women with T2DM.15 Metformin was associated with a significantly higher incidence of gastrointestinal disturbance, but with no serious maternal or fetal adverse effects. 16-18
According to the consensus statement of the American Diabetes Association (ADA), it is premature to claim that metformin has been shown to be safe and effective in pregnancy.19 There may be specific circumstances when metformin is continued or started during pregnancy, but this decision should be made with a woman giving informed consent after discussing the limitations of current data.19,20 Likewise, a 2006 review of metformin treatment in pregnancy found insufficient evidence of safety and did not recommend routine treatment with the drug.32 The use of metformin for women with anovulatory PCOS has no benefit with respect to enhancing either fertility or live-birth rates, and its routine use is not recommended. 3
During the last decade, several retrospective and non-randomized studies have evaluated metformin for its potential disease-modifying effects. Studies have shown that without metformin, spontaneous abortion may occur in 25% to 73%21-23 of pregnancies than the general population. The increased risk may be due to hyperandrogenism, high LH level, more insulin resistance and higher levels of plasminogen activator inhibitor activity (PAI-1) which adversely affects endometrial function and environment.21,23,24 Because metformin reverses the adverse endocrine and metabolic risk factors for miscarriage in PCOS (insulin resistance, elevatedPAI-1 and androgens), metformin should theoretically reduce the incidence of first trimester spontaneous abortion. Metformin treatment in the pregnant PCOS patients resulted in significant decrease in miscarriage rate.7,23,25 However, there is a lackof robust data indicating the true live birth rates in women with PCOS when metformin is used as first line treatment.15
Gestational diabetes (GDM), defined as any degree of glucose intolerance whose first diagnosis is during pregnancy, affects around 4-7% of pregnancies. The link between PCOS and gestational diabetes was initially suggested by several retrospective series.26-28 Women with PCOS who are insulin resistant are at high risk for the development of diabetes in pregnancy. In a large population based study, GDM has been reported to affect up to 18% of patients diagnosed with PCOS with an odds ratio of 2.4.40 A meta-analysis by Boomsma demonstrated that PCOS was independently associated with an increased risk for gestational diabetes and hypertension after the confounding factors such as body mass index (BMI) were taken into consideration. 29 A possible role for metformin therapy may be the prevention of GDM. The study by Glueck has shown that use of metformin 2.55g/day among PCOS patients throughout pregnancy was associated with a 10-fold reduction in GDM (31% versus 3%). It also reduces insulin resistance and insulin secretion, thus decreasing the secretory demands imposed on pancreatic beta-cells by insulin resistance and pregnancy.15 Likewise, in the study by De Leo (metformin 1700 mg-3g/day)7 and Khattab (metformin 1-2g/day),30 resulted in a reduction in gestational diabetes among those who were treated with metformin than among those normal pregnant controls [(0 versus 13%, p <0.005) and (OR=0.17, 95% CI 0.07,0.37) respectively]. However, given the lack of data from well-designed, prospective clinical trials, metformin is currently not indicated for the prevention of GDM.
Contrary to previous reports indicating beneficial effects of metformin in pregnant PCOS, a large randomized trial on metformin treatment from first trimester to delivery does not show any benefit of the drug in terms of gestational diabetes, preeclampsia, preterm delivery or the composite of these three pregnancy complications.18 The study by Vanky did not address the possible effect of metformin on early pregnancy loss or the benefits of continuing metformin after pregnancy is confirmed.18 Moreover, a meta-analysis of randomized, controlled trials demonstrated no effect of metformin on abortion rate (OR=0.89; 95% CI 0.59,1.75; p=0.9).31
Despite conflicting data, some physicians still use metformin to facilitate fertility and reduce pregnancy complications such as gestational diabetes, pregnancy-induced hypertension, preterm births and miscarriage. At present, there is no local study on the use of metformin among pregnant women with PCOS specifically addressing the maternal and neonatal outcomes during pregnancy.
This study will help elucidate the role of metformin among pregnant Filipino women with PCOS, specifically to determine the maternal outcome among pregnant women with PCOS on metformin treatment in terms of: rate of first trimester spontaneous abortion, development of gestational diabetes, pregnancy-induced hypertension, age of gestation and modes of delivery. This study also aimsto determine the neonatal outcome among pregnant women with PCOS on metformin treatment in terms of: live birth rates, APGAR score, birth weight and congenital anomalies . We compared the pregnancy outcomes of the women who became pregnant while taking metformin and remained on metformin throughout pregnancy versus the pregnancy outcomes of the women who discontinued metformin at the time the pregnancy was confirmed.
A retrospective cohort study was performed to determine the pregnancy outcome on the use of metformin on women diagnosed with PCOS. Data collection through review of outpatient records was carried out. All subjects were seen at a private infertility clinic of St. Luke’s Medical Center, Quezon City from year 2004 to 2012. Patients whose records were incomplete were contacted by telephone to supply missing data. To be included in the study, the subject must be diagnosed with PCOS and be on metformin treatment prior to becoming pregnant. All patients met the PCOS criterion of the Rotterdam ESHRE/ASRM consensus (two of the following three manifestations: irregular or absent ovulation, elevated levels of androgenic hormones, and/or enlarged ovaries containing at least 12 follicles each).3 None of the women had diabetes mellitus prior to achieving pregnancy. Patients with known hyperprolactinemia, thyroid disease, pituitary insufficiency, intake of medications such as steroid, oral contraceptive pills and thiazolidenediones were excluded.
The following independent variables were recorded: name, age at diagnosis of PCOS, family history of diabetes (type 1 or 2), pre-existing medical conditions (diabetes, hypertension, dyslipidemia, allergy, asthma etc.), number of years diagnosed with PCOS, pre-pregnancy weight/height/BMI, years of infertility, baseline investigations (pelvic ultrasound, fasting plasma insulin, FBS or OGTT, total testosterone, SHBG, LH/FSH ratio, 17 hydroxy-progesterone, prolactin, thyroid function tests), duration of metformin therapy, dose of metformin therapy and continuation of metformin use into pregnancy (weeks AOG).
The following dependent variables were recorded: GDM as measured by 75g or 100g OGTT at first prenatal check up and at 24-28 weeks, blood pressure measurements, ultrasound assessment for fetal growth and anatomic abnormalities at 22 to 24 weeks gestation, gestational age during delivery (preterm/term/post-term delivery), manner of delivery (vaginal, caesarean), pregnancy outcome (alive, fetal demise), APGAR Score at 5 minutes and maturity testing (full term/premature).
All women were followed up and treated during pregnancy withstandard antenatal care. Clinical care was provided by a single obstetrician, who used metformin along with assisted reproductive technologies (ART) to facilitate fertility and to treat polycystic ovary syndrome, and whose practice is to continue metformin throughout pregnancy with the intent to avoid gestational diabetes, pregnancy-induced hypertension, preterm births and spontaneous abortion. All of the pregnant PCOS women were offered metformin after a thorough explanation of the risks and benefits by the attending physician.
Evaluation during pregnancy: Pregnancy was confirmed by urine pregnancy test or plasma ß-human chorionic gonadotropin(ß-hCG) and detection of gestational sac in the uterine cavity by ultrasonography. Congenital scan was performed using ultrasound at 22 to 24 weeks age of gestation. All women repeated the 100-g or 75-g oral glucose tolerance test between 24 to 28 weeks of pregnancy as screening for gestational diabetes.
Determination of miscarriage: Women with symptoms suggestive of miscarriage (e.g., vaginal bleeding, abdominal pain) documented and confirmed by transvaginal ultrasonography.
Assuming that the incidence of GDM among pregnant women who take metformin is 13% and among those who do not take metformin is 30%, with an alpha error of 0.05, power of 80% and 1 tailed alternative hypothesis, the calculated sample size was 71 for each group or 142 for both groups.
The women were divided into two groups: first, women who continued metformin during pregnancy and second, women who discontinued metformin at the time the pregnancy was confirmed.
Description of qualitative data was done by the use of percentages or proportion. Quantitative data were described using the mean and the standard deviation. Determination of the effect of metformin on maternal and neonatal outcomes was analyzed using chi-square test. And finally, determination of factors related to spontaneous abortion was analyzed using multiple logic regression. Level of significance (alpha) was set at 0.05.
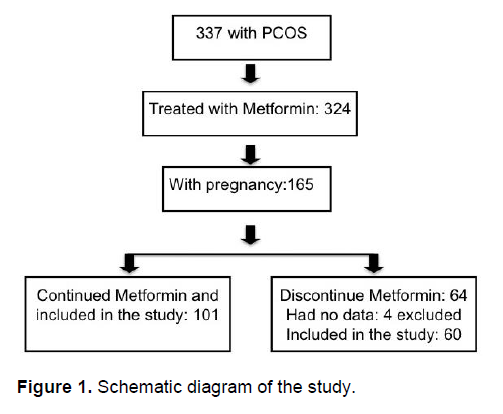
A total of 337 non-diabetic women fulfilled the criteria for PCOS. Of these, 324 women were treated with metformin. One hundred sixty five women conceived and served as the participants of the study. These women became pregnant while taking metformin together with different assisted reproductive techniques (ART) such as ovulation induction, intrauterine insemination or in vitro fertilization (IVF). Of the 165 patients who met the inclusion criteria, 101 patients continued metformin during pregnancy and 60 women immediately discontinued metformin at the time the pregnancy was confirmed. The remaining 4 patients had incomplete data. Women who discontinued metformin either elected not to use the drug and opted for dietary modification alone or transferred to the care of another physician. Among those who continued metformin during pregnancy, 4 of these women reported gastrointestinal side effects and eventually discontinued metformin between 20 to 32 weeks gestation while the rest continued metformin up to delivery (See Figure 1).
Click here to download Figure 1
Figure 1. Schematic diagram of the study.
The usual starting dose of metformin among these women is 500 mg tablet twice a day titrated gradually up to 2000 to 2500 mg tablet per day depending on the patient’s drug tolerability. The metformin dose in the majority of this cohort of women ranged between 1500 to 1850 mgs once daily.
Click here to download Table 1
Table 1. Pre-conception clinical characteristics of PCOS women
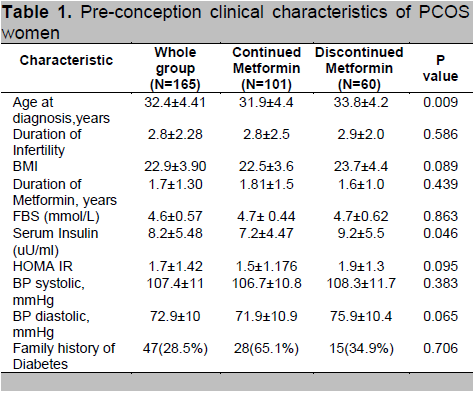
Table 1 shows the pre-conception clinical characteristics of the 165 PCOS women prior to metformin treatment, and who either continued taking metformin during pregnancy (continued metformin, n=101) and those that discontinued metformin at the time the pregnancy was confirmed (discontinued metformin, n=60). The result did not significantly differ in the pre-pregnancy variables between the two groups, except for the age of diagnosis of PCOS and fasting insulin levels.
Click here to download Table2
Table 2. Maternal outcome among pregnant PCOS
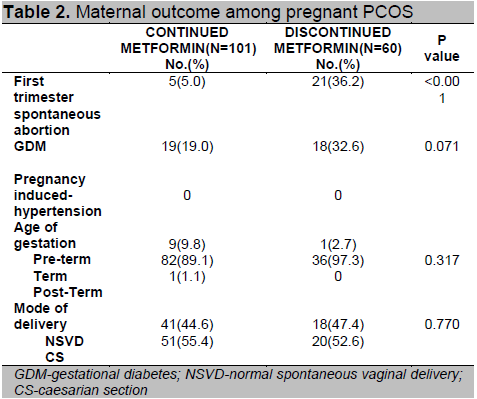
Table 2 shows that there was a smaller proportion of women who had a first trimester spontaneous abortion among those who continued metformin compared to those who discontinued metformin during pregnancy (5% versus 36.2%). The difference is statistically significant (p < 0.001). Those given metformin during pregnancy had GDM in 19% of cases compared to 32.6% among those that did not continue metformin. None in either group developed pregnancy-induced hypertension. Most pregnancies ended in term delivery (> 37weeks’ gestation), half of them delivered by spontaneous vaginal delivery and the other half by caesarean section. All of these variables did not reach statistical significance except for spontaneous abortion.
Table 3. Using multiple logistic regression analysis, those who took metformin during pregnancy had 0.168 times the odds of having spontaneous abortion compared to those who discontinued metformin (OR=0.168; 95% CI 0.048,0.592; p=0.005). Other variables such as age and fasting insulin levels were not significantly related with spontaneous abortion.
Click here to download Table 3
Table 3. Multivariate analysis on the effect of metformin during pregnancy on spontaneous abortion
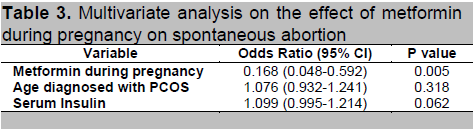
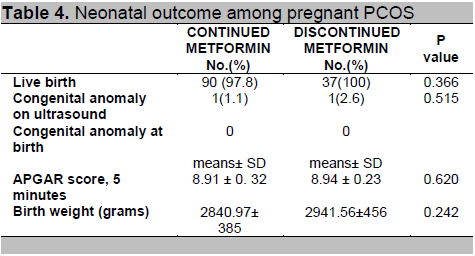
Table 4. The differences in neonatal outcomes between the two groups did not achieve statistical significance.
Click here to download Table 4
Table 4. Neonatal outcome among pregnant PCOS
The observed reduction in the rate of spontaneous abortion, defined as miscarriage during the first trimester, in this study (36.2% vs 5%) is in agreement with the previous studies showing a beneficial effect of metformin in reducing spontaneous abortion. Two studies have shown that treatment with metformin significantly lowers the rate of abortion in women with PCOS (the metformin-treated groups experienced approximately one-third the miscarriage rates of the control groups).15,33 The early pregnancy loss rate among those who discontinued metformin is comparable with the 30 to 50% rate of early pregnancy loss of clinically recognized pregnancies after either spontaneous or assisted conception, a rate three-fold higher than that reported for normal women.34
The effect of metformin on spontaneous abortion is controversial.The beneficial effect may be due to the favorable effect of metformin on plasminogen activator inhibitor, thus improving implantation12,15,21 or to metformin’s ability to increase uterine blood flow.23 Furthermore, some studies suggest that hyperinsulinemia decreases the expression of glycodelin and IGF-binding protein-1. Glycodelin may play a role in inhibiting the endometrial immune response to the embryo and IGF binding protein-1 appears to facilitate adhesion processes at the feto-maternal interface. 35,36
Multiple studies have documented the link between high BMI and higher fetal loss rate,22 probably linked to a higher insulin resistance among these obese women. Although many women with PCOS are obese, obesity is not a part of the diagnostic criteria for PCOS. The disease has multiple phenotypes, women who are lean can also have PCOS. The cohort of women in this study has normal weight (mean BMI 22.9 kg/m2 ± 3.90) based on the Asia Pacific consensus on obesity, with a mean pre-pregnancy HOMA-IR value >1.4 for both groups. This may indicate insulin resistance based on a local study by Yu-Mallen et al.32 It seems that metformin is capable of decreasing the rate of fetal loss by a mechanism independent of its effect on maternal body weight.
In a study comparing three groups of women with PCOS on metformin, all rates of miscarriage were reduced while on metformin treatment, however the groups that stopped at 8 weeks and 12 weeks had a statistically significant decrease in the miscarriage rates (from 40 % to 8%, and from 32% to 4%, respectively) while the group that discontinued metformin immediately after the pregnancy was confirmed did not have a statistically significant drop.42 On the contrary, the report by Palomba, a meta-analysis of randomized controlled trials, showed that preconception intake of metformin did not have a beneficial effect on reducing miscarriage rates in women with PCOS.31
Metformin administration during pregnancy is suggested to reduce the risk of gestational diabetes15 despite conflicting systematic reviews on the topic.18,39 Our study showed a modest, near significant trend toward decreasing the development of gestational diabetes among those women who continued metformin during pregnancy as compared to those who discontinued metformin after pregnancy was confirmed. An editorial by Legro39 regarding the study by Vanky et al.18 showed that metformin initiated during the first trimester and continued until delivery did not improve overall rates of gestational diabetes. Legro stated that the study cohort was a relatively healthy group of women with PCOS who had probably no real need for metformin. There was a relative lack of obesity in the women at baseline, and by using the Rotterdam criteria for the diagnosis of PCOS, the study likely included less metabolically challenged patients.39 Similarly to this study, our result may not be generalizable to other more obese, glucose-intolerant populations with PCOS.
Since metformin modulates blood pressure, insulin resistance and fibrinolytic activity, it is reasonable to assume that it may prevent gestational hypertension and preeclampsia. Most studies reporting an association between hypertension or pre-eclampsia and pregnancy in PCOS show mixed results. 28 In our study, none of the PCOS women developed gestational hypertension with or without metformin treatment. The study by Mikola showed that PCOS was not a significant predictor of pre-eclampsia compared with control pregnancies.27 Glueck et al15 have prospectively compared the prevalence of pre-eclampsia in 90 PCOS women treated with metformin compared to 252 healthy controls and showed no difference was observed between the two groups (5.2% vs 3.6% respectively). These findings are congruent with the study of Vanky, which concluded that metformin treatment from first trimester to delivery did not reduce pregnancy complications in PCOS including preeclampsia.18, 39
With regards to neonatal outcome, all neonates had appropriate growth for gestational age. The mean neonatal APGAR score at 5 minutes, birth weight and infant birth rates were comparable between the two groups. A recent meta-analysis of insulin sensitizers for the treatment of infertility in PCOS concluded that the use of metformin for improving reproductive outcomes in women with PCOS appears to be limited and that there was no evidence that metformin improved live birth rates whether it was used alone (OR=1.00; 95% CI 0.16 to 6.39) or in combination with clomiphene (OR= 1.05; 95% CI 0.75 to 1.47). 16
Gilbert38 evaluated the prevalence of major fetal malformations among neonates exposed to metformin during the first trimester. In their meta-analysis, the malformation rate in the metformin group was 7.2% versus 1.7% in the control. Review articles by Koren41 in five separate cohort studies in 2006 showed that the rate of congenital abnormalities does not increase with metformin. In our study, one subject showed a dilated left third ventricle on congenital anomaly scan, indicating agenesis of the corpus callosum in the metformin group. The infant was carried to term and delivered without any other major complications. No hydrocephalus or other major congenital anomalies at birth was noted.
The main limitation of this paper is its retrospective nature and the small sample size.
A similar study with a longer follow-up period is recommended in order to further assess the neonatal outcome beyond the first week of life. A randomized, placebo-controlled, double blind clinical trial will be required to optimally confirm the spontaneous abortion-sparing capability of metformin. Until then, the option to continue or discontinue metformin during pregnancy remains controversial. Clinicians must counsel pregnant women with PCOS appropriately before initiation of metformin therapy.
In women with PCOS, continuous use of metformin during pregnancy significantly reduced the rate of first trimester spontaneous abortion. A smaller proportion of pregnant PCOS patients developed GDM when they continued metformin treatment throughout pregnancy compared to those who did not. Neonatal outcomes were not significantly affected by metformin treatment.
1. Frank S. Polycystic ovary syndrome. N Engl J Med. 1995; 333: 853-856.
2. Asuncion M, Calvo RM, San Millan JL, Sancho J, Avila S, Escobar Morreale HF. A prospective study of the prevalence of the polycystic ovary syndrome in unselected Caucasian women from Spain.J Clin Endocrinol Metab. 2000;85:2434-243.
3. Fauser B, TarlatzisB,RebarR,Legro R, et al.Consensus on women’s health aspects of polycystic ovary syndrome (PCOS): The Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Fertility and Sterility. 2012; 97(1):0015-0282.
4. Hellmuth E, Damm P, Molstead-Pedersen L. Oral hypoglycemic agents in 118 diabetic pregnancies. Diabet Med. 2000;17(7):507-511.
5. Conway GS, Agrawal R, Betteridge DJ, Jacobs HS. Risk factors for coronary artery disease in lean and obese women with the polycystic ovary syndrome. Clin Endocrinol. 1992; 37: 119-125.
6. Dunaif A, Segal KR, Futterweit W. Dobrjansky A. Profound peripheral insulin resistance, independent of obesity, in polycystic ovary syndrome. Diabetes. 1989;38:1165-1174.
7. De Leo V, Musacchio MC, Piomboni P, Sabatino AD. The administration of metformin during pregnancy reduces polycyctic ovary syndrome related gestation complications. Euro Jour of Obstretrics&Gyneco and Reproductive Biology. 2011;157: 63-66.
8. Gilbert C, Valois M, Koren G. Pregnancy outcome after first-trimester exposure to metformin: A meta-analysis. Fertil Steril. 2006;86:658-663.
9. Ehrmann DA. Polycystic ovary syndrome. N Engl J Med. 2005;352:1223-1236.
10. Moghetti P, Castello R, Negri C, Tosi F, Caputo M, Zanolin E and Muggeo M. Metformin effects on clinical features, endocrine and metabolic profiles, and insulin sensitivity in polycyctic ovary syndrome: A randomized, double blind, placebo-comtrolled 6-month trial, followed by open, long-term clinical evaluation. J Clin Endocrinol. Metab. 2000;85:139-146.
11. Glueck CJ, Wang P, Fontaine R, Tracy T, Sieve-Smith L. Metformin-induced resumption of normal menses in 39 of 43 (91%) previously amenorrheic women with polycystic ovary syndrome. Metabolism. 1999;48:511-19.
12. Glueck CJ, Wang P, Fontaine R, Tracy T, Sieve-Smith L. Metformin to restore normal menses in oligo-amenorrheic teenage girls with polycystic ovary syndrome. J Adol Health. 2001;29:160-69.
13. Piacquadio K, Hollingsworth DR, Murphy H. Effects of in-utero exposure to oral hypoglycemic drugs. Lancet. 1991;338(8771):866-869.
14. Vanky E, Zahlsen K, Spigset O, Carlsen SM. Placental passage of metformin in women with polycystic ovary syndrome. Fertil Steril. 2005;83:1575-1578.
15. Glueck CJ, Wang P, Kobayashi S, Phillips H, Sieve-Smith L. Metformin therapy throughout pregnancy reduces the development of gestational diabetes in women with polycystic ovary syndrome. Fertil Steril. 2002; 77: 520-525.
16. Tang T, Lord JM, Norman RJ, Yasmin E, Balen A. Insulin-sensitizing drug (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndorme, oligo amenorrhoea and subinfertility.Cochrane Database Syst Rev. 2010;(1):CD003053.
17. Legro RS, Barnhart HX, Schlaff WD. Clomiphene, metformin, or both for infertility in the polycyctic ovary syndrome. N Engl J Med. 2007;356:551-566.
18. Vanky E, Stridsklev S, Heimstad R, Romundastad P. Metformin versus placebo from first trimester to delivery in polycystic ovary syndrome: A randomized, controlled multicenter study. J Clin Endocrinol Metab. 2010; 95(12):E448-455.
19. American Diabetes Association. Metformin in Pregnancy. Diabetes Care.2006; 29:2.
20. Thessaloniki ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Consensus of infertility treatment related to polycystic ovary syndrome. Fertil Steril. 2008;89:505-522.
21. Glueck CJ, Philipps H, Cameron D, Sieve-Smith L. and Wang, P. Continuing metformin throughout pregnancy in women with polycyctic ovary syndrome appears to safely reduce first-trimester SAB: A pilot study. Fertil Steril. 2001;75:46-52.
22. Wang JX, Davies MJ and Norman RJ. Polycystic ovarian syndrome and the risk of spontaneous abortion following assisted reproductive technology treatment. Hum Reprod. 2001;16:2606-2608.
23. Jakubowicz DJ, Iuorno MJ, Jakubowicz S, Roberts KA. Effects of metformin on early pregnancy loss in the polycystic ovary syndrome. J. Clin Endocrinol Metab. 2002;87:5077-511.
24. Norman RJ, Wang JK, Hague W. Should we continue or stop insulin-sensitizing drugs during pregnancy? Curr Opin Obstet Gynecol. 2004;16:245-250.
25. Glueck CJ, Wang P, Goldenberg N, Sieve-Smith L. Pregnancy outcomes among women with PCOS treated with metformin. Human Reproduction. 2002;17:2858-2864.
26. Holte J, Gennarelli G, Wide L. et al. High prevalence of polycystic ovaries and associated clinical, endocrine, and metabolic features in women with previous gestational diabetes mellitus. J. Clin. Endocrinol. Metab. 1998;83:1143–1150.
27. Mikola M, Hiilesma V, Halttunen M et al. Obstetric outcome in women with polycystic ovary syndrome. Hum Reprod. 2001;16:226-229.
28. Haakova L, Cibula D, Rezabek K, Hill M, Fanta M, Zivny J. Pregnancy outcome in women with PCOS and in controls matched by age and weight. Hum Reprod. 2003;18(7):1438-1441.
29. Boomsma CM, Eijkemans MJ, Hughes EG Visser GH, Fauser BC, Macklon NS. A meta-analysis of pregnancy outcomes in women with polycystic ovary syndrome. Hum Reprod Update. 2006;12(6):673-683.
30. Khattab S, Mohsen IA, Aboul Foutouh I, Ashmawi HS, Mohsen MN et al. Can metformin reduce the incidence of gestational diabetes mellitus in pregnant women with polycystic ovary syndrome? Prospective cohort study. Gyne Endocrinol. 2011;27(10):789-793.
31. Palomba S, Falbo A, Orio F Jr, Zullo F.Effect of preconceptional metformin on abortion risk in polycystic ovary syndrome: A systematic review and meta-analysis of randomized controlled trials. Fertil Steril. 2009;92(5):1646-1658.
32. Lilja AE, Mathiesen ER. Polycystic ovary syndrome and metformin in pregnancy.Acta obstetrician et gynecologica Scandinavica. 2006.85 (7): 861-868.
33. Khattab S, Mohsen IA, Ramadan A, Moaz M, AI- Inany H. Metformin reduces abortion in pregnant women with polycystic ovary syndrome. Gynecol Endocrinol. 2006;22: 680-684.
34. Homburg R, Armar NA, Eshel A, Adams J, Jacobs HS. Influence of serum LH concentrations on ovulation, conception, and early pregnancy loss in polycystic ovary syndrome.BMJ. 1998;297:1024-1026.
35. Fedorcsak P, Storeng R, Dale PO, Tanbo T, Abyholm T. Obesity is a risk factor for early pregnancy loss after IVF or ICSI. Acta Obstetric Gynecology Scand. 2000;79:43-48.
36. Jakubowicz DJ, Seppälä M, Jakubowicz S, Rodriguez-Armas O, Rivas-Santiago A, Koistinen H, et al. Insulin reduction with metformin increases luteal phase serum glycodelin and insulin-like growth factor-binding protein concentration and enhances uterine vascularity and blood flow in the PCOS. J Clin Endocrin Metab. 2001;86:1126-1133.
37. Yu-Mallen L, Tan-Garcia J, Gaston J, Quimpo J. Prevalence of insulin resistance as determined by HOMA assessment with PCOS at St. Luke’s Medical Center: Phil. J. Internal Medicine. 2004;42:233-241.
38. Gilbert C, Valois M, Koren G. Pregnancy outcome after first-trimester exposure to metformin: A meta-analysis. Fertil Steril. 2006;86:658-663.
39. Legro R. Metformin during Pregnancy in Polycystic Ovary Syndrome: Another Vitamin Bites the Dust. J. Clin Endocrinol Metab. 2010;95(12):5199-5202.
40. Lo J, Feigenbaum S, Escobar G. Increased Prevalence of Gestational Diabetes Mellitus Among Women with Diagnosed Polycystic Ovary Syndrome: A population-based study. Diabetes Care. 2006; 29: 1915-1917.
41. Koren G, Gilbert C, Valois M. Metformin use during first trimester of pregnancy. Is it safe? An Fam Physician. 2006;52:171-172.
42. Sohrabvand F, Shariat M, Haghollahi F, Bagheri B. Effect of metformin on miscarriage in pregnant patients with polycystic ovary syndrome. West Indian Med J. 2009; 58(5):433-436.
Articles and any other material published in the JAFES represent the work of the author(s) and should not be construed to reflect the opinions of the Editors or the Publisher.
Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.