Pituitary Hyperplasia and Van Wyk Grumbach Syndrome: A Consequence of Chronic Untreated Congenital Hypothyroidism
Deep Dutta, Manoj Kumar, Rajesh Jain, Anubhav Thukral, Sujoy Ghosh, Satinath Mukhopadhyay, Subhankar Chowdhury
Deep Dutta, MD
Room-9A, 4th floor Ronald Ross Building
Department of Endocrinology and Metabolism
IPGMER & SSKM Hospital
244 AJC Bose Road, Calcutta-700020, India
Tel. No.: +919477406630
Fax No.: +913322236558
E-mail: deepdutta2000@yahoo.com
e-ISSN 2308-118x
Printed in the Philippines
Copyright © 2013 by the JAFES
Received March 24, 2013. Accepted April 23, 2013.
Keywords: primary hypothyroidism, Van Wyk Grumbach Sundrome, precocious puberty
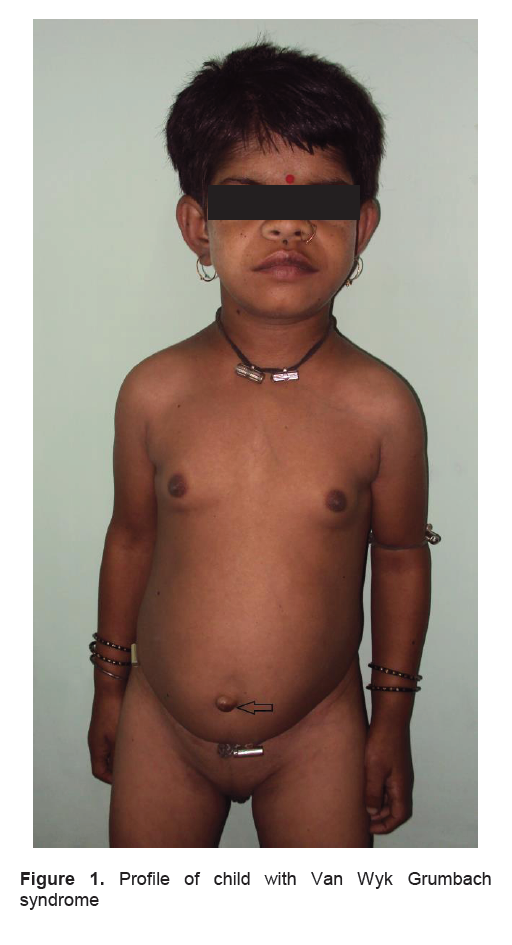
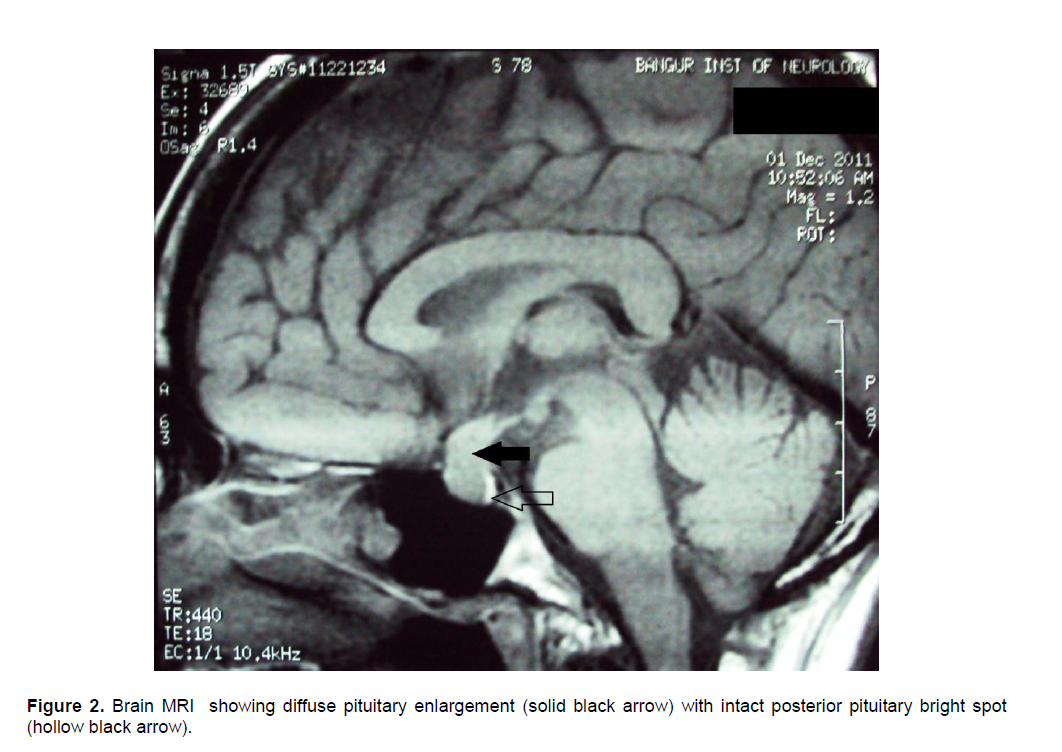
An eight-year, 4-month old Indian girl with low IQ and delayed milestones, presented with headache (4 years), breast development (4 months), and menstrual bleeding for 22 days. Examination revealed short stature [height: 91.5 cm; SD score: -5.59], coarse dry skin, umbilical hernia (arrow), delayed reflexes, Tanner’s stage-3 breasts, absent pubic and axillary hair. Investigations revealed delayed bone age (3 years), enlarged ovaries with multiple follicles, free T4 <0.35ng/dl (0.9-1.9), TSH 75μU/ml (0.4-4.2), prolactin 323ng/ml (2.5-17), LH <0.1U/L (1.14-5.75), FSH 3.2U/L (1.37-13.56), estradiol 28pg/ml (prepubertal<5pg/ml) and anti-thyroid peroxidase antibody 21U/L (<34). LH and FSH, 40 minutes post 100μg triptorelin were pre-pubertal (0.9U/L and 5.8U/L respectively). Brain MRI revealed diffuse pituitary enlargement. She showed clinical improvement with levothyroxine replacement with resolution of headache, cessation of menstrual bleed, mild decrease in breast size, normalization of TSH, prolactin and 15 cm height gain in 15 months since treatment initiation.
Van Wyk Grumbach syndrome (VWGS)1 is GnRH independent precocious puberty, believed to be due to TSH mediated activation of gonadal FSH receptor (in the setting of chronic TSH elevation secondary to chronic untreated primary hypothyroidism) resulting in increased estrogen leading to breast development, ovarian follicular cysts and menstruation in the absence of pubic and axillary hair development which are dependent on adrenal androgens.2 Hormonal overlap at the level of G-protein coupled receptors due to common α-subunit between TSH and FSH is the underlying principle.3 TRH mediated reversible thyrotroph and lactotroph hyperplasia explains the pituitary enlargement and headache in these children. 4
Click here to download Figure 1
Figure 1. Profile of child with Van Wyk Grumbach syndrome
Click here to download Figure 2
Figure 2. Brain MRI showing diffuse pituitary enlargement (solid black arrow) with intact posterior pituitary bright spot (hollow black arrow).
1. Van Wyk JJ, Grumbach MM. Syndrome of precocious menstruation and galactorrhoea in juvenile hypothyroidism: An example of hormonal overlap in pituitary feedback. Journal of Pediatrics 1960;57:416–435.
2. Ryan GL, Feng X, d’Alva CB et al. Evaluating the roles of follicle-stimulating hormone receptor polymorphisms in gonadal hyperstimulation associated with severe juvenile primary hypothyroidism. Journal of Clinical Endocrinology and Metabolism. 2007; 92:2312–2317.
3. Kroeze WK, Sheffler DJ, Roth BL. G-protein-coupled receptors at a glance. Journal of Cell Science. 2003; 116:4867–4869.
4. Jawadi MH,Ballonoff LB, Stears JC, Katz FH. Primary hypothyroidism and pituitary enlargement. Radiological evidence of pituitary regression. Arch Intern Med. 1978; 138:1555-1557.
Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.