Metastatic Adenocarcinoma Arising from Fibrocalcific Pancreatic Diabetes
Deep Dutta, Manoj Kumar, Rajesh Jain, Anubhav Thukral, Dibakar Biswas, Sujoy Ghosh, Satinath Mukhopadhyay, Subhankar Chowdhury
Deep Dutta, MD
Room 9-A, 4th floor Ronald Ross Building
Department of Endocrinology and Metabolism
IPGMER & SSKM Hospital
244 AJC Bose Road, Calcutta-700020, India
Tel. No.: +919477406630
Fax No.: +913322236558
E-mail: deepdutta2000@yahoo.com
e-ISSN 2308-118x
Printed in the Philippines
Copyright © 2013 by the JAFES
Received May 17, 2013. Accepted October 9, 2013.
Keywords: fibrocalcific pancreatic diabetes, carcinoma, pancreas, screening
Fibrocalcific pancreatic diabetes (FCPD) is a rare form of ketosis-resistant diabetes in the young (15 to 40 years old) of unknown etiology. It has been observed in tropical and subtropical countries with highest incidence in south India, and is believed to have some association with tropical chronic pancreatitis, malnutrition, toxin exposure (e.g., cassava) and SPINK1 mutation. It is associated with a hundredfold increased risk of pancreatic cancer compared to the general population.1-3
Click here to download Figure 1
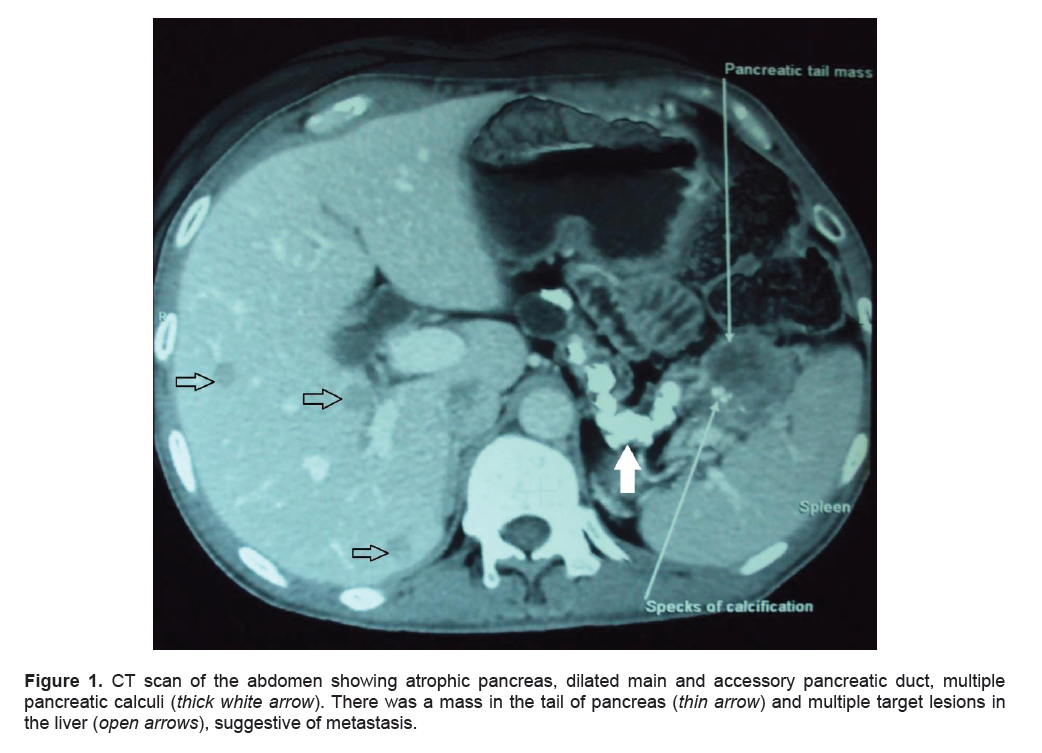
Figure 1. CT scan of the abdomen showing atrophic pancreas, dilated main and accessory pancreatic duct, multiple pancreatic calculi (thick white arrow). There was a mass in the tail of pancreas (thin arrow) and multiple target lesions in the liver ( open arrows), suggestive of metastasis.
Click here to download Figure 2
Figure 2. Photomicrograph of the liver from Tru-cut biopsy in hematoxylin and eosin stain showing metastatic adenocarcinoma. Abnormal cells appear to have increased nucleocytoplasmic ratio and prominent nuclei along with nucleoli (solid black arrow), in the background of large eosinophilic cells with small nucleus characteristic of hepatocytes (hollow black arrow).
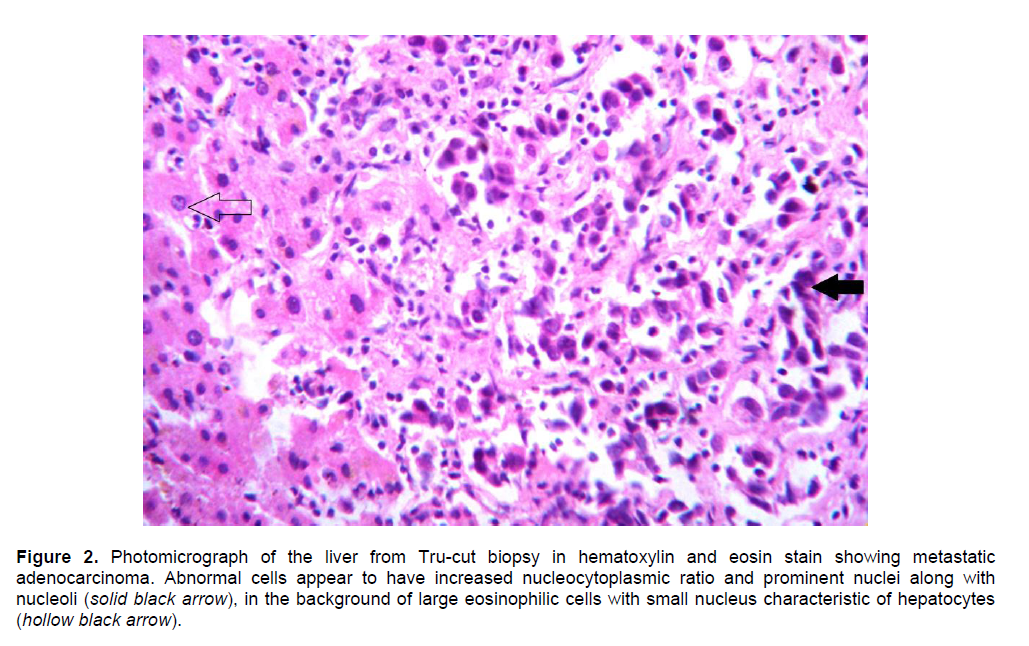
A 43-year-old diabetic male presented with recurrent abdominal pain since 24 years of age, anorexia and weight loss of 8 kg in the last 6 months. Computerized tomography (CT) revealed multiple calculi in the pancreatic head, body and tail; a 38 mm x 38 mm x 32 mm mass in the pancreatic tail; and multiple target lesions in the right lobe of liver (Figure 1). He was diagnosed of diabetes at 28 years age, which was well controlled with glimepiride and metformin. In the last 2 years, the patient was shifted to premixed insulin and subsequently multiple subcutaneous insulin injections due to worsening glycemic control, and was on 58 units insulin/kg/day. His HbA1c at the time of admission was 9.6%. Serum CA19-9 was elevated (828.8 U/L, normal value <40 U/L). Tru-cut biopsy of the right lobe of liver revealed moderately differentiated metastatic adenocarcinoma (Figure 2).
CA19-9 is elevated in 70 to 80% of patients with pancreatic cancer. It is predictive of distant metastasis or disease recurrence.4 Consensus statements have recommended screening for pancreatic cancer in any individual with an increased risk (more than 10-fold), which includes individuals with at least 3 first-degree relatives with pancreatic cancer, Peutz-Jeghers syndrome, familial atypical multiple mole melanoma and hereditary pancreatitis. 4,5 The association between FCPD and carcinoma of the pancreas is not well-known, with some reports suggesting that patients with FCPD may be at higher risk. This warrants further studies to evaluate cancer risk, and to develop screening tools for early detection of malignancy.3
1. Bhatia E, Choudhuri G, Sikora SS et al. Tropical calcific pancreatitis: Strong association with SPINK1 trypsin inhibitor mutation. Gastroenterology 2002;123(4):1020-5.
2. Braganza JM, Sherry J, Indira P et al. Xenobiotics and tropical chronic pancreatitis. Int J Pancreatology 1990:222–45.
3. Chari ST, Mohan V, Pitchumoni CS et al. Risk of pancreatic carcinoma in tropical calcific pancreatitis: An epidemiologic study. Pancreas 1994;9(1):62-6.
4. Chakraborty PP, Dutta D, Biswas K et al. Pancreatic carcinoma in fibrocalcific pancreatic diabetes: An eastern India perspective. Indian J Endocrinol Metab 2012;16(Suppl 2):S486-8.5. Chong I, Cunningham D. Pancreatic cancer. In: Longo DL, Fauci AS, Kasper DL et al., eds. Harrison's Principles of Internal Medicine. Vol. 1. 18th ed. McGraw Hill; 2012:786-90.
Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.