Remarkable Calcifications in Medullary Thyroid Carcinoma
Mukut Roy, Pranab Kumar Sahana, Nilanjan Sengupta, Chanchal Das, Ranen Dasgupta
Mukut Roy, MD
Department of Endocrinology
Nilratan Sircar Medical College, Kolkata
West Bengal, India
Tel. No.: +919748683932
E-mail: mukutdoc@gmail.com
e-ISSN 2308-118x
Printed in the Philippines
Copyright © 2013 by the JAFES
Received July 29, 2012. Accepted: October 9, 2013.
Keywords: Medullary Thyroid Carcinoma, Thyroid ultrasound, Calcifications
Various patterns of calcifications may be seen in thyroid cancers on ultrasonography (USG) of thyroid.1 Coarse calcifications seen in medullary thyroid carcinoma (MTC) are generally associated with posterior shadowing on thyroid ultrasound.2 We briefly report this case of MTC with an emphasis on its radiological features.
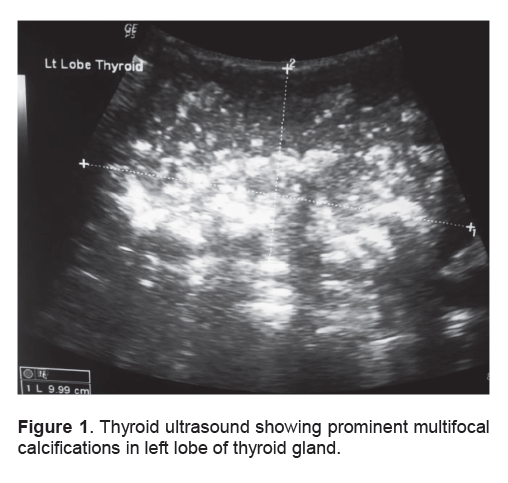
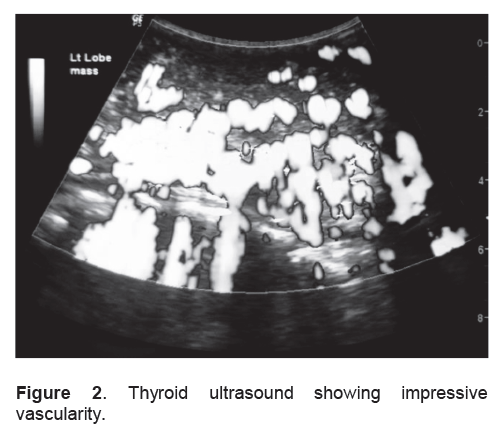
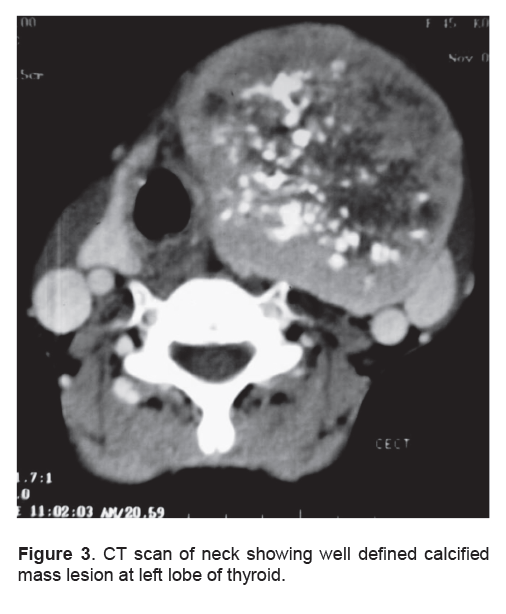
A 45-year-old post-menopausal female presented with a goiter (8 cm × 7 cm) of ten years duration. History was uneventful otherwise. Thyroid function tests were: free T3-2.20 pg/ml (ref. range: 1.71- 3.71), free T4-1.18 ng/100ml (ref. range: 0.7-1.48) and TSH-1.42 µIU/ml (ref. range: 0.35-4.94) respectively. Subsequently, thyroid ultrasound revealed prominent calcifications and increased vascularity (Figure 1), (Figure 2). Computed Tomography (CT) scan of neck showed large (80 mm × 78 mm) well defined, calcified mass lesion in the left lobe of the thyroid (Figure 3). Fine needle aspiration biopsy (FNAB) confirmed evidence of MTC. A highly elevated calcitonin (20,000 pg/ml) (ref. range: < 5 pg/ml) was consistent with the diagnosis of MTC.
Click here to download Figure 1
Figure 1 . Thyroid ultrasound showing prominent multifocal calcifications in left lobe of thyroid gland.
Click here to download Figure 2
Figure 2 . Thyroid ultrasound showing impressive vascularity.
Click here to download Figure 3
Figure 3 . CT scan of neck showing well defined calcified mass lesion at left lobe of thyroid.
MTC may be associated with dense, irregular foci of calcifications which are in contrast with homogeneous calcifications of other thyroid tumors. 2,3 MTC, first described by Hazard et al.4 in 1959, has become the focus of increasing clinical and experimental investigations. However, in thyroid carcinomas, ultrasonographic evidence of an abundance of calcifications may be rarely seen nowadays due to improved health awareness and earlier diagnosis. To conclude, in an asymptomatic patient with long standing goiter, coarse macrocalcifications in imaging findings should make the physician vigilant in ruling out MTC.
1. Taki S, Terahata S, Yamashita R et al. Thyroid calcifications: Sonographic patterns and incidence of cancer. Clin Imaging. 2004; 28: 368-371.
2. Gorman B, Charboneau JW, James EM. Medullary thyroid carcinoma: Role of high-resolution US. Radiology. 1987; 162: 147-150.
3. McCook TA, Putman CE, Dale JK, Wells SA. Medullary carcinoma of the thyroid: Radiographic features of a unique tumor. Am J Roentgenol. 1982; 139: 149-155.
4. Hazard JB, Hawk WA, Crile G. Medullary (solid) carcinoma of the thyroid: A clinicopathologic entity. J Clin Endocrinol Metab. 1959; 9: 152-161.
5. Yanhua Bai, Gengyin Zhou, Misa Nakamura, Takashi Ozaki, Ichiro Mori, Emiko Taniguchi et al. Survival impact of psammoma body, stromal calcification and bone formation in papillary thyroid carcinoma. Modern Pathology. 2009; 22 : 887–894.
Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.