Rodolfo F. Florentino, MD, PhD
Chairman-President
Nutrition Foundation of the Philippines
18 May Street, Congressional Village, Quezon City
Tel. No.: +63 926 7838
E-mail: rfflorentino@yahoo.com
e-ISSN 2308-118x
Printed in the Philippines
Copyright © 2011 by the JAFES
Received August 14, 2011. Accepted October 5, 2011.
Developing countries around the world – including those in Asia – are in a state of rapid economic transition as a result of generally improving incomes, increasing industrialization, urbanization, and globalization. This state has given rise to changing lifestyle and diets, from one with high level of physical activity and diets based mostly on plant foods, to one with a higher level of sedentariness, and a diet of increasing energy density, fat and animal foods and less plant foods – a state of nutrition transition.1 This in turn has led to an increase in overweight and obesity especially in adults, and a consequent rise in chronic diseases such as cardiovascular disease, hypertension, Type 2 diabetes and other so-called “diseases of affluence.” At the same time in these countries, the high rate of undernutrition especially in children remains the major nutrition problem even if it has somewhat improved, resulting in a situation where undernutrition persists at the same time with increasing overnutrition, a phenomenon now known as the dual burden of malnutrition.2 This situation could be observed within the country, as well as within communities and even in the same household. While undernutrition results in poor growth, stunting and poor resistance to infection in children, and low physical and mental performance in both children and adults, overnutrition results in obesity and its well-established co-morbidities. Moreover, severe nutritional deprivation in fetal and early post-natal period followed by a rapid catch-up growth in early childhood is now known to increase the risk of overweight and obesity, as well as cardiovascular disease, diabetes and other chronic diseases in adolescence and adulthood – following the so-called “Barker hypothesis. “3 Such a situation calls for over-arching policies, strategies and programs to counter this dual threat to overall health and thus to socio-economic development.
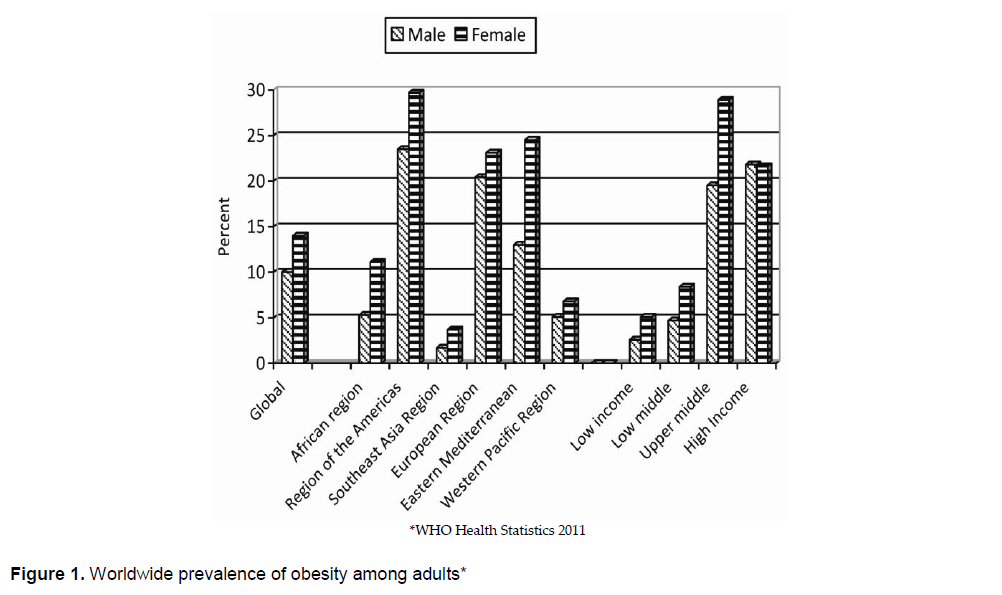
According to the World Health Organization, the global prevalence of obesity in 2008 was as high as 10.0% among males and 14.0% among females, lowest among the low income countries and highest among the high income countries4 (Figure 1). While the Asian regions, namely, Southeast Asia and Western Pacific, showed the lowest prevalence of obesity among the WHO regions, the prevalence of undernutrition in these two regions was the highest among the regions.
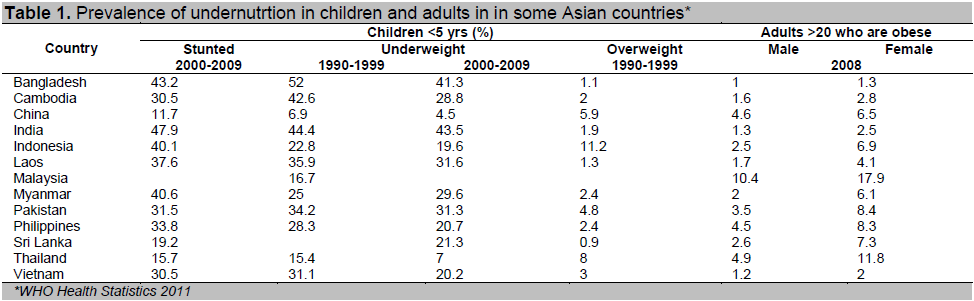
In developing countries in Asia, stunting among children <5yrs ranged from 11.7% to 47.9% and underweight ranged from 4.5% to 43.5% during the decade 2000-2009 (Table 1). However, it could be seen that there were rather large differences among countries in the region, more or less following the state of economic development. In India, the prevalence of underweight children <5 yrs was 43.5% during the 2000-2009 and that of obesity among adult males and females only 1.3% and 2.5%, respectively, in 2008. On the other hand in Malaysia, the prevalence of underweight children <5 yrs was only 16.7% during the 2000-2009, that of obesity among adult males and females was as high as 10.4% and 17.9%, respectively, in 2008. While in Bangladesh, the prevalence of underweight children <5 yrs was 52.0% during the 2000-2009 and that of obesity among adult males and females was only 1.0% and 1.3%, respectively, in 2008, in China, the prevalence of underweight children <5 yrs was only 6.9% during the 2000-2009 and that of obesity among adult males and females was as high as 4.6% and 6.5%, respectively, in 2008. Except for the Pacific island countries like Fiji and Kiribati where the prevalence of obesity is very high, and Japan where the prevalence is very low, the other countries in the region - Cambodia, Laos, Vienam, the Philippines, Indonesia, Thailand, Pakistan and Sri Lanka - more or less followed a similar trend. It also important to note that the rates of undernutrition among children has slowly decreased in these countries from the decade 1990-1999 to 2000-2009, while the rates of obesity, although relatively low, have dramatically increased. As a whole, the double burden of malnutrition is evident among developing countries in Asia.
The latest National Nutrition Survey conducted in the Philippines in 20085 (Table 2) gives an even clearer picture of the double burden of malnutrition in an average developing country.
Click here to download Figure 1
Figure 1. Worldwide prevalence of obesity among adults*
Click here to download Table 1
Table 1. Prevalence of undernutrtion in children and adults in in some Asian countries*
Click here to download Table2
Table 2. Prevalence of malnutrition among children, adolescents and adult Filipinos, 2008*
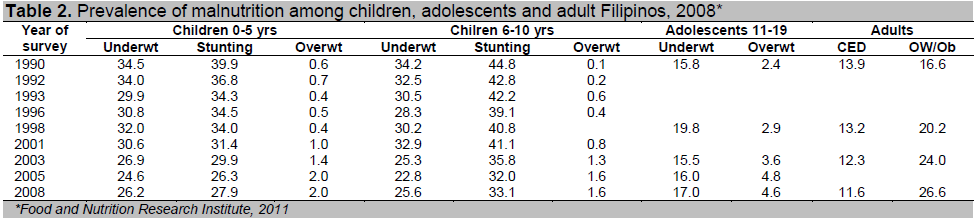
The 2008 National Nutrition Survey conducted by the Food and Nutrition Research Institute, Department of Science and Technology, covered a random sample of 36,634 households and their members, from all regions of the Philippines. Among the 0-5 yr old children, the prevalence of underweight-for-age was 26.2%, that of stunting, 27.9%, and that of overweight-for-age, 2.0% in 2008. The prevalence of underweight and stunting generally declined from 1990 (34.5% and 39.9%, respectively) to 2008. On the other hand, the prevalence of overweight increased from 0.6% to 2.0% during the same period. Among the 6-10 yr old children, the prevalence of underweight-for-age was 25.6% in 2008, that of stunting was 33.1%, and that of overweight-for-age was 1.6%. (Table 2) The survey also showed a reduction in the prevalence of undernutrition in this age group from that in 1990 (34.2% underweight and 44.8% stunting). On the other hand there was an increase in overweight from 0.1% in 1990 to 1.6% in 2008. The rate of overnutrition in children may still be low, but the four-fold to sixteen-fold rate of increase in prevalence is significant. Among adolescents, the prevalence of underweight (by BMI-for-age) was 17.0%, while those at risk of overweight was 4.6% in 2008. Among adults, 20 yrs and over, the prevalence of chronic energy deficiency (BMI <18.5) in 2008 was 11.6%, a slight reduction from 13.9% in 1993. On the other hand, the prevalence of overweight (BMI ≥25) was 26.6%, a large increase from 16.6% in 1993.
The dual burden of malnutrition has also been clearly noted even in poorer countries in the region like India and Bangladesh.
With the on-going socio-economic transition in India, accompanied by the demographic and health transition and changing food supply and consumption patterns, dual burden of malnutrition has been clearly seen in national nutrition surveys in India.6 Over the last three decades, there has been a decline in prevalence of both moderate and severe malnutrition including stunting, although the prevalence of underweight and stunting among pre-school children is still unacceptably high. In adults, there has also been a progressive decline in the prevalence of undernutrition and “some increase” in overnutrition in both urban and rural areas. While significant differences in under- and overnutrition could be seen among the states, overnutrition and obesity are emerging as major problems in all states. A study by Subramanian,7 however, has shown that dual malnutrition is not apparent in very low socio-economic groups.
Studies by Shafique et al in Bangladesh8 have also shown that double burden of malnutrition exists in both rural and urban poor women. While chronic energy deficiency (CED) continued to be prevalent among Bangladeshi women, 9.1% of urban poor and 4.1% of rural women were overweight (BMI ≥25) between 2000 and 2004. During this period, the prevalence of CED decreased (urban poor, from 33.8%n to 29.3%; rural, from 42.6% to 36.6%) but the prevalence of overweight increased (urban poor, from 6.8% to 9.1%; rural, from 2.8% to 5.5%).
Two nationally representative surveys in Vietnam conducted by the National Institute of Nutrition in Hanoi9, one in 2000 and the other in 2005, also showed a double burden of malnutrition in adults, although there was a shift toward a higher BMI level between the two surveys. The prevalence of overweight increased from 3.5% to 6.6% nationwide, while that of underweight declined although still high, in 2005.
More recently, it has been shown that double burden of malnutrition occurs not only within the country as a whole, but also within households. This phenomenon has attracted many investigators trying to understand the factors for its occurrence.
Analysis of the 1993 China Health and Nutrition Survey involving 3349 household by Doak, et al10 revealed 8.1% of all households with underweight and overweight members within the same household. Urban residence and high income were significantly associated with the presence of both forms of malnutrition in the same household. Such households were more likely to own modern appliances such as television, motor vehicle, and washing machine, and more likely to consume a higher percentage of energy from fat and protein than the normal weight households.
The same group of investigators11 analyzed national surveys conducted between 1988 and 1996 from Brazil, China, Indonesia, the Kyrgyz Republic, Russia, Vietnam and the United States. In six of the countries studied, 22-66% of households had both underweight and overweight persons coexisting in the same household. They also found that the dual burden households was more likely to be urban and of higher income and in countries in the middle range of GNP. In Vietnam and Indonesia, 60% and 40%, respectively of households with an overweight person also had an underweight person.
Garrett and Ruel12 analyzed 42 Demographic and Health Surveys in Africa, Asia and Latin America conducted between 1992 and 2001. They found that the prevalence of pairs of stunted child and overweight mother was less than 10% among the Asian countries studied. It was, more prevalent in the urban areas in Bangladesh, India and Nepal, and more prevalent in the rural areas in Cambodia, Kazakhstan, Kyrgyz Republic and Uzbekistan, showing that the phenomenon is not necessarily urban. However, the prevalence was found to increase with economic development, and in countries in the midst of nutrition transition.
As part of a multi-center study in Asia on the problem of dual forms of malnutrition in the same household, Agdeppa et al13 did a study of dual forms of malnutrition in Tondo, Manila. They found that 59% of child-mother pairs were suffering from the two forms of malnutrition, and of this, 8.2% child-mother pairs in the same household had an underweight child and an overweight mother. An in-depth study of these under/overweight child-mother pairs showed that this phenomenon was associated with mother’s educational level, mother’s occupation, energy intake, the preference of meats sweets and sugars among children, or meats and fried foods among mothers.
In the same series of multi-center studies in Asia, Khor and Shariff14 reported their case study of this phenomenon among poor Malay rural households. Out of 140 households studied, 52.1% of mothers were overweight, 15.7% of the children 1-6 yrs were underweight, 27.1% were stunted and 5% wasted. The children from normal weight child-mother pairs had significantly higher intake of total calories, fat and riboflavin than children from underweight children/overweight mother pairs. Mean energy and nutrient intake of mothers from both groups were not significantly different. The study confirmed that inadequate intake of total energy and nutrients as the major factor for underweight children in this community. In another study in Malaysia among indigenous people, Saibul et al15 found that while food variety may predict a healthier diet in children, it may increase the risk of overweight and obesity in adults.
From national surveys and local studies, it is clear that most countries in Asia suffer from dual burden of malnutrition: on the one hand an unacceptably high rate of undernutrition in the form of underweight and stunting in children and chronic energy deficiency in adults, and on the other hand, a growing rate of overnutrition in the form of overweight and obesity in both children and adults. In fact, in a significant percentage of households, both undernutrition and overnutrition are found at the same time in the same household, for example, an undernourished child and an overweight mother. Both forms of malnutrition constrain the development of the full potential of individuals, communities and nations. Undernutrition affects physical and mental health and performance throughout the lifespan, while overnutrition gives rise to an increasing rate of chronic diseases occurring at earlier and earlier ages. It is becoming clear that this phenomenon arises from a common set of social and economic factors operating in the individual, local and national levels. It is imperative, therefore, to re-examine the current policies, strategies and programs directed to the improvement of nutrition of the population, from one that addresses each form of malnutrition independently, to one where both forms are addressed simultaneously and seen from a holistic perspective. Policies and intervention programs will need to encompass a wide range of sectors, political, economic, agriculture, education, health and industry, involving governments, community and the private sector. Above all, a strong political will based on a full understanding of this dual burden of malnutrition is the key to success.
1. Popkin BM. The nutrition transition and obesity in the developing world. J Nutr. 2001; 131:871A-973S.
2. Gillespie S. Haddad L: Attacking the double burden of malnutrition in Asia and the Pacific. Washington DC: Asian Development Bank, Philippines and International Food Policy Research Institute: 2001.
3. Barker DJ. The effect of nutrition of the fetus and neonate on cardiovascular disease in adult life. Proc Nutr Soc. 1992;51:135-44.
4. WHO Health Statistics 2011. www.who.int /whosis/whostat/ EN_WHS2011_Full.pdf.
5. Food and Nutrition Research Institute. The Seventh National Nutrition Survey. FNRI-DOST, 2011, Taguig City, Philippines.
6. Nutrition Foundation of India. Double burden of malnutrition. Case Study from India. FAO Food and Nutrition Paper. 84. 2003.
7. Subramanian SV, Perkins JM and Khan KT. Do burdens of underweight and overweight co-exist among lower socio-economic groups in India? Am J Clin Nutr. 2009;90:369–76.
8. Shaffique S, Akhter N, Stallkamp B, de Pee S, Panagides D and Bloem M. Trends in under- and overweight among rural and urban poor women indicate the double burden of malnutrition in Bangladesh. Int J Epid. 2007;16:449-457.
9. Ha DTP, Feskens EJM, Deurenberg P, Mai LB, Khan NC and Kok FJ. Nationwide shifts in the double burden of underweight and overweight in Vietnamese adults in 2000 and 2005: Two national nutrition surveys. BMC Public Health. 2011;11:62.
10. Doak C, Adair L, Bentley M, Fengying Z, and Popkin B. The underweight/overweight household: An exploration of sociodemographic and dietary factors in China. Public Health Nutrition. (2002) 5;215-221.
11. Doak CM, Adair LS, Bentley M, Monteiro, C and Popkin BM. The dual burden household and the nutrition transition paradox. Int J Obesity. 2005;29:129-136.
12. Garrett JL and Ruel MT. Stunted child-overweight mother pairs: Prevalence and association with economic development and urbanization. Food and Nutrition Bulletin. 2005; 26:209-221.
13. Agdeppa IA, Lana RD and Barba CVD. A case study of dual forms of malnutrition among selected households in District 1, Tondo, Manila. Asia Pacific J Clin Nutr. 2003;12 (4): 438-446.
14. Khor GL and Sharif ZM. Dural forms of malnutrition in the same households in Malaysia – A case study among Malay Rural households. Asia Pacific J Clin Nutr. 2003;12 (4): 427-438.
15. Saibul N, Sharif ZM, Khor GL, Kandiah M, Ghani NA and Rahman HA. Food variety score is associated with dual forms of malnutrition in Orang Asli (Malaysian endogenous peoples) householdsL Implications for health promotion. Asia Pac J Clin Nutr. 2009;18 (3):412-422.