Graves’ disease is an autoimmune disorder characterized by thyrotoxicosis, enlarged thyroid gland and ophthalmopathy. It affects various organs and tissues in the body.[1] Without treatment, complications such as infertility, cachexia, cardiac arrhythmias, cardiomyopathy, thyroid storm and even death can result.[2]
Aside from the complications of the disease, hyperthyroid Graves’ patients often have neuropsychiatric complaints including memory problems, emotional lability, irritability, depression and anxiety that can negatively impact quality of life. Quality of life improves after treatment once euthyroid state is achieved.[3]
The goal of therapy is to correct the hypermetabolic state by keeping T4 and/or T3 levels within normal range with the fewest side effects and the lowest incidence of hypothyroidism. Three modalities are commonly used to treat Graves’ hyperthyroidism: antithyroid drugs (ATD), surgery, or radioiodine (RAI) ablation.
ATD therapy inhibits thyroid hormone synthesis with preservation of the thyroid gland. Maximum remission or cure rates (i.e., permanent resolution of hyperthyroidism defined by normalization of T4 and/or TSH levels off ATDs) of up to 60% are achieved with 18–24 months of continued use. With ATD discontinuation, hyperthyroid relapse rate is up to 50%. There is no permanent hypothyroidism with this mode of treatment and for unclear reasons, the relapse rates appear to vary in different geographic regions. In a study made by Tütüncü et al., in Turkey (an iodine deficient country) remission rate decreased from 74.4% to 65.1% in the first year and after four years, thereafter. The long-term remission is not predicted by the remission achieved in 2 years’ time in areas low in iodine.[4] Patients with severe hyperthyroidism and large goiters are likely to relapse when treatment is stopped, but outcome is difficult to predict. The common side effects of ATD are rash, urticaria, and arthralgia (1–5%). Rare but major side effects include hepatitis, an SLE-like syndrome and agranulocytosis (<1%).[5]
Rarely resorted to nowadays due to its cost and invasive nature, subtotal or near-total thyroidectomy is only considered for patients with very large, nodular goiters or those who relapse after anti-thyroid drugs, and based on patient’s personal preference over RAI.
RAI ameliorates hyperthyroidism by permanent destruction of thyroid tissue. It is effective with remission or cure rates reaching up to 80%. It is gaining popularity as first line therapy since it is effective, safe, and easy to administer; except for contraindication to its use in pregnant and lactating women, and some controversies surrounding its use in individuals under 20 years old. Hyperthyroidism may persist for 2–3 months before radioiodine takes full effect. Persistent hyperthyroidism is usually treated with a second dose of radioiodine 6-12 months after the first dose.[6]
However, RAI usually leads to permanent hypothyroidism regardless of dosage thereby necessitating long-term thyroxine replacement in majority of patients. The risk is at least 10–20% in the first year and 5% per year thereafter. Up to 90% become hypothyroid in 25 years.[7] Efforts to calculate an optimal dose of radioiodine that achieves euthyroidism without a high incidence of hyperthyroid relapse or progression to hypothyroidism have not been successful. Due to this, many authorities currently favor an approach aimed at early permanent hypothyroidism as opposed to euthyroidism to avoid missing the diagnosis of hypothyroidism later on.
Moreover, in 15 percent of patients, Graves’ ophthalmopathy can develop or get worse with use of radioactive iodine.
Anti-thyroid drugs are the predominant therapy in many centers in Europe and Japan, whereas radioiodine is more often the first line of treatment in North America. (Published data as to which treatment modality is preferred in our country is still unavailable.) These differences reflect the fact that no single approach is optimal, each has its own advantages and disadvantages.[8] Assessment of physical, social function, mental health and overall well being is, therefore, an important outcome when treating patients with this disease.
In a study by Watt et al., involving interviews with 80 thyroid outpatients, 21 of whom had Graves’ disease, to identify how thyroid diseases impact the patients’ lives and to select the most relevant quality of life issues for a thyroid-specific questionnaire, broader quality-of-life domains were chosen to be most relevant, especially fatigue, emotional susceptibility and impact on daily life.
In a prospective randomized open label trial by Torring, et al., involving 119 Swedish patients with Graves’ disease age 33-55 years old randomly assigned treatment with either methimazole 10mg QID + LT4 100-300mcg/day + B-blocker 18 months then withdrawn (medical group), subtotal thyroidectomy + LT4 replacement (surgical group) or RAI using calculated dosimetry accounting for thyroid size and 24hr RAIU (RAI group). The cure rates at second year, which was their primary outcome, was 66% for the medical group, 79% for RAI and 92% for surgical group. Part of their secondary outcome included an assessment of the patients’ views of the disease and treatment using a non-validated disease-specific questionnaire administered 3 years after the initiation of treatment. Ninety percent of the subjects in all groups were satisfied with the treatment they received, although around 30% from each arm still felt that they have not recovered even after a year. The number of sick leaves within 2 years from treatment was not statistically different among the three groups.[9]
Thyroid disease-specific quality-of-life patient-reported outcome (ThyPRO) measure was developed by Watt et al. The ThyPRO questionnaire initially has 85 items which encompass quality of life across benign thyroid diseases. The questionnaire was cross-culturally validated and currently exists in 7 translated languages namely: English, Dutch, Serbian, Italian, Indian, Danish and Swedish.[10]Utilizing the ThyPRO, the Serbian version showed that Graves’ disease patients had significant improvement in their quality of life after surgery.
Before, the Short Form 36 (SF-36) Health Survey was used for benign thyroid disorders. It is a generic measure and may not target a specific disease.[11] For example, SF-36 does not include goiter symptoms. The only available HRQoL related to thyroid pathology is the validated questionnaire for differentiated thyroid cancer.[12]
There are no published questionnaire to assess quality of life of Graves’ disease patients after receiving ATD or RAI in the Philippines, so a questionnaire should first be developed and validated. The assessment by comparison of quality life is the primary objective of this study and the assessment tool used is the ThyPRO originally made by Watt et al. To date, the comparison under these treatments has not yet been made to cases of Graves’ disease patients. This small scale pilot study may serve as a guide for future large scale or multicenter study in the country with the use of culturally adapted benign thyroid disease questionnaire. Locally adapted tool will fit our local demographics adding acceptability of the assessment and evaluation of quality of life. This locally adapted tool is the ThyPROph.
In treatment of patients with benign thyroid disease, the decision for medical therapy with anti-thyroid drug or RAI depends on the balance between the benefits of being cured of hyperthyroidism and the risk of permanent hypothyroidism leading to lifetime thyroxine replacement. The patient's question about how much better he is likely to feel may be relevant to his decision as well. Information about the impact of the different treatment modalities on health-related quality of life (HRQoL), therefore, will aid clinicians in helping patients make a fully informed choice hence this study.
METHODOLOGYStudy Design and Population
The study has 2 phases. First phase is the translation and validation wherein cross-sectional analytical design was used. Second phase of the study is the comparison of quality of life scores with RAI treatment versus ATD wherein cross-sectional comparative study design was used.
The study was conducted after being approved by the University of Santo Tomas Hospital Institutional Review Board (USTH-IRB). The subjects participated after signing informed consent. The identity and other information about the respondents in the study were kept strictly confidential.
First Phase: Translation and ValidationAdult euthyroid Graves’ disease patients consulting at the private and clinical division of the University of Santo Tomas Hospital (USTH) were recruited. Inclusion criteria included patients with Graves’ disease who were already euthyroid (TSH + T4 or fT4 within normal ranges taken at least 2 months from date of study inclusion) for at least 6 months after RAI or after ATD treatment. Exclusion criteria included those with thyrotoxic cardiomyopathy, thyrotoxic hypokalemic periodic paralysis, pregnant or breastfeeding individuals and those who were unable to read Tagalog or English.
Description of the Study Population The QuestionnaireThe ThyPRO 39 which is a shorter version of the original ThyPRO questionnaire was utilized in this study. The original ThyPRO questionnaire was developed by Torquil Watt et al., in Denmark and published at European Journal of Endocrinology in 2010. The questionnaire was utilized with permission from the tool developer with approval and response received through e-mail.[3] The questionnaire consisted of 12 scales and 1 about Impact on overall QoL. Questions included 3 goiter symptoms, 4 hyperthyroid symptoms, 4 hypothyroid symptoms, 3 eye symptoms, 3 on tiredness, 3 on cognitive complaints, 3 on anxiety, 3 on depression, 3 on emotional susceptibility, 3 on impaired social life, 3 on impaired daily life, 3 on appearance and finally 1 about Impact on overall QoL. The item is rated on a 0-4 Likert scale with choices as follows: not at all, a little, some, quite a bit and very much. Table 1 shows the scale content of the ThyPRO questionnaire.
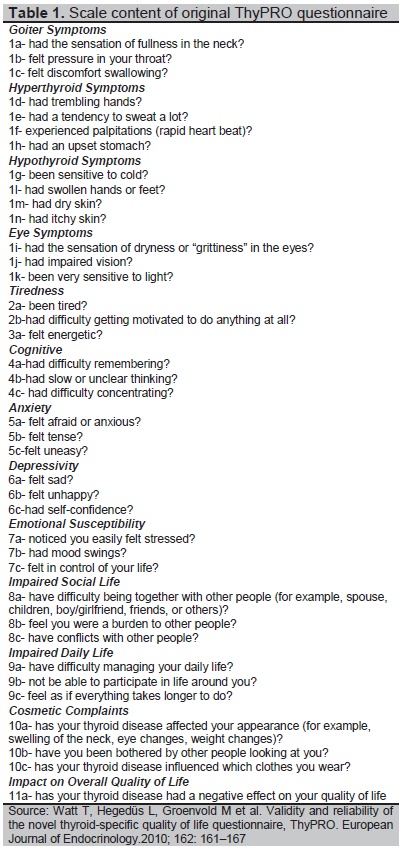
Table 1. Scale content of the original ThyPRO questionnaire
A. Translation Process
In the translation process, one Filipino teacher was asked to translate the questionnaire from English to Tagalog (forward translation 1) with the aid of the investigator. Another Filipino teacher was called upon for translation from English to Filipino as well (forward translation 2). The two translators compared the versions and agreed on a common Filipino version of the questionnaire. An English teacher served as third translator. The Filipino version was translated back to English (back-translated version). The study adviser identified and commented on differences between the original English questionnaire and the Filipino version. Suggestions were made on how this will be handled.
After approval of the study adviser, the translated ThyPRO questionnaire was presented to 2 endocrinology consultants, 2 endocrinology fellows, 1 nurse and 2 non-medical/lay persons for review for comprehensibility of the questionnaire to both medical and non-medical/lay persons. After which, the suggestions of the review committee were carried out by the study adviser and the second edited ThyPRO Filipino version was derived. .
B. PretestingThe translated ThyPRO questionnaire was pre-tested to 5 actual patients who had hyperthyroidism before and had either medical treatment or radioactive iodine. They were asked if the questionnaire was clear and if changes were necessary. Final revision of ThyPRO Filipino version questionnaire was made to arrive at draft ThyPRO Filipino version.
C. Validation of the DRAFT ThyPRO Filipino version QuestionnaireTwenty subjects who fulfilled the inclusion criteria were asked to answer the pre-final ThyPRO Filipino version questionnaire for validation.
Assessment of validity of the pre-final ThyPRO Filipino version questionnaire was accomplished using following measures: content, internal consistency/reliability and construct validity.
- Content validity was measured with the assessments made by the endocrine consultants and fellows, and the pretesting results of 5 patients.
- Internal consistency was assessed using Cronbach’s alpha. Acceptable consistency will be an alpha value of >0.7. Cronbach’s alpha is a measure of relationships of the items in the questionnaire as a group.
- Construct validity was assessed using convergent and discriminant validity. Spearman’s rho was determined for convergent validity and Inter-Item correlation (IIC) was computed for the discriminant validity. IIC result less than 0.85 tell us that discriminant validity likely exists between the scales.
The same inclusion and exclusion criteria were used for the second phase of the study.
Sample Size CalculationCurrently, no study comparing the quality of life of those who underwent RAI or on ATD is available in the Philippines. As a preliminary data and in this pilot study, the following formula will be used for sample size calculation:
n= ln (1-ϒ)/ln (1-π)
where ln means logarithm, ϒ is confidence level set at 95% and π is the probability level set at 5%. Based on the above formula the sample size in this study is 58 patients with Graves’ disease.
Statistical AnalysisSPSS was used for statistical analysis. Means and range summarized the data in quantitative form. While counts and percentages were used for qualitative data. Differences between demographic profiles, such as gender, marital status, educational attainment, employment and goiter grade (categorical variable) were compared using Chi-Square Test; while numerical variable (age, disease duration, initiation of treatment) were compared using Independent T-test. Comparison of Quality of Life scores was done using independent t-test. Correlation of the domains with the demographics was determined using Pearson correlation coefficient (for numerical variable) and Spearman rank signed test (for categorical variable). P-value of 0.05 is considered in this study.
First Phase: Translation and Validation Content Validation
The following are the output of the review committee together with the adviser which provided content validity:
Item 1a: The consensus on translation for the “fullness in the neck” is “paninikip ng leeg” instead of “kapunuan sa leeg.”
Item 1b: The “pressure in your throat” is translated simply to “bara sa lalamunan” instead of “bigat/bara sa lalamunan.”
Item 1f: Instead of using the Taglish “palpitasyon,” pagkabog sa dibdib was used.
Item 2b: The English version was translated as “nawalan ng gana sa kahit anong gawain.”
Reliability and ValidityThe internal consistency or reliability of the scales was assessed using Cronbach’s alpha where a value of >0.7 is consistent with good internal consistency or reliability. The Cronbach’s alpha reliability of the 13 items ranged from -0.153 to 0.854. Scale on Impaired Social Life and Anxiety shows an acceptable degree of internal consistency, with Cronbach’s alpha of 0.854 and 0.784, respectively. However, poor internal consistency for ThyPRO Filipino version are classified on the scales on Eye Symptoms (α=0.198), Emotional Susceptibility (α=-0.153), Cosmetic Complaints (α=0.286), Tiredness (α=0.312), Hypothyroid (α=0.499) and Hyperthyroid (α=0.270) Symptoms, Cognitive (α=0.515), Depressivity (α=0.369), Impaired Daily Life (α=0.601). Despite the outcomes of the internal consistency reliability per scale, overall the ThyPRO Filipino version has an acceptable degree of internal consisteny with Cronbachs’s alpha of 0.839 (Table 2). This is comparable to the original study wherein the Cronbach alpha is greater than 0.7.
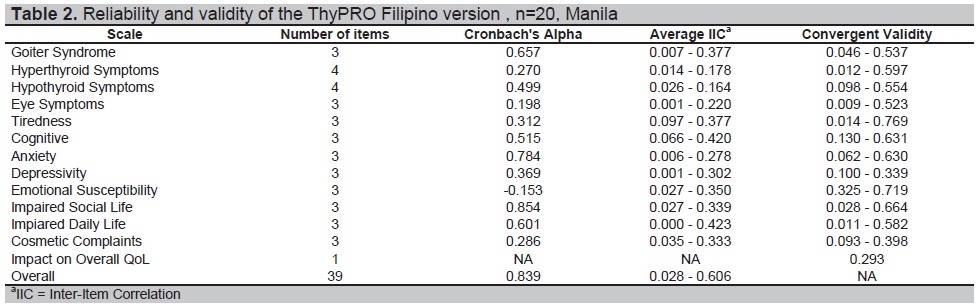
Table 2. Reliability and validity of the ThyPRO Filipino version, n=20, Manila
Discriminant validity and convergent validity were used to assess the construct validity of the ThyPROph. Convergent validity measures the degree of confidence that the trait is well measured by its indicators; while discriminant validity is the degree to which measures of different traits are unrelated. The convergent validity calculated using Spearman correlation ranged from rs=0.014–0.769. Majority of the scales of the questionnaire had a moderate correlation with Spearman correlation above rs=0.40. The scale Emotional Susceptibility has convergent validity ranges from adequate (rs=0.325) to high correlation (rs=0.719). The scales Tiredness, Cognitive and Impaired Social Life has poor to high correlation of rs=0.014–0.769, rs=0.130–0.631 and rs=0.028–0.664 respectively. Only the scale Depressivity has poor to adequate correlation (rs=0.100–0.339)
Based on the discriminant validity of the scales, an average Inter-Item Correlation (IIC) result less than 0.85 tell us that discriminant validity likely exists between the scales. The discriminant validity of the scales in the questionnaire ranged between IIC=0.001 and IIC=0.423. Cognitive scale obtained an IIC=0.066–0.420; while Impaired Daily Life scale, ICC=0.000–0.423. Moreover, overall divergent validity of the ThyPRO is adequate to excellent with IIC=0.028–0.606. Since the computed IIC is below 0.85, discriminant validity exists between the different scales of ThyPROph. This is comparable to 0.77-0.89 intraclass correlation in the original study. The different scales theoretically measure different constructs from one another. Therefore, the different scales are unrelated from one another.
Second Phase of the Study: Comparison of quality of life scores with RAI treatment versus ATD Demographic Profile of RespondentsFifty-eight patients with Graves’ disease completed the ThyPROph with 48.28% (n=28) under the RAI group, and 51.72% (n=30) under ATD group. The mean age of the patients under ATD group is higher than the RAI group, but statistically not significant (44.52 y.o. vs 41.82 y.o. respectively, p=0.4535). There were more females in the ATD group (83.33% vs 64.29%). Moreover, there were more singles (50%), high school graduates (46.43%) and employed subjects (57.14%) in the RAI group. Looking at the ATD group, majority were married (60%), high school graduates (46.67%) and unemployed (56.57%). Despite such differences, marital status (p=0.2320), educational attainment (p=0.8010) and employment status (p=0.2930) were not significantly different between groups. Distribution of goiter grading between groups were also not significantly different with both groups having more subjects with Grade 0 goiter (89.29% and 70%) (Table 3).
A significant difference is seen in disease duration (p=0.0027) and initiation of treatment (p=0.0120). Disease duration corresponds to the time the patient was diagnosed to have Graves’ disease until the time the patient was seen by the investigator. The RAI group was diagnosed to have Graves’ disease at a mean of 8.97 years with initiation of RAI at a mean of 7.76 years. In the ATD group, disease duration also parallels the initiation of treatment.
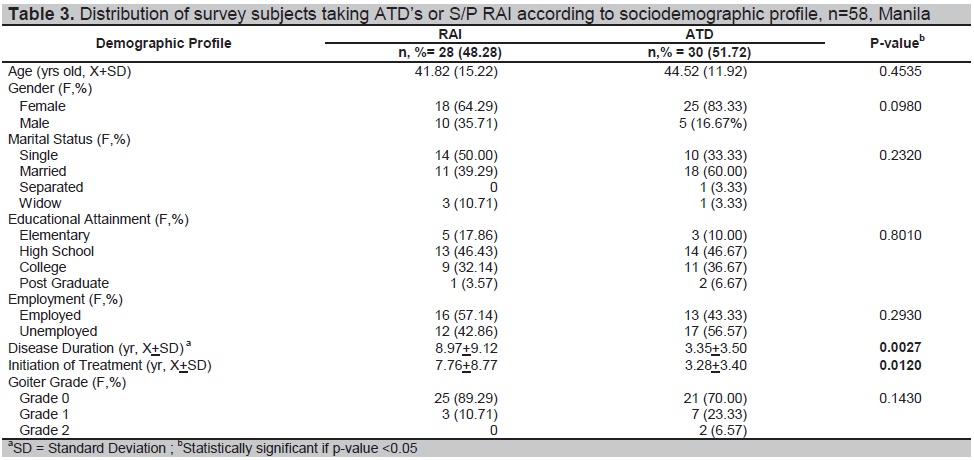
Table 3. Distribution of survey subjects taking ATD’s or S/P RAI according to sociodemographic profile, n=58, Manila
Health Related Quality of Life of Filipino Patients with Graves’ Disease
In determining HRQoL of patients with Graves’ disease, the scores of each domain were computed based on the ThyPRO scoring system. The lower the score, the better or more improved is the quality of life. There is a significant difference in the domains “goiter symptoms” (p=0.0209), “emotional susceptibility” (p=0.0067) and “impaired daily life” (p=0.0463). The HRQoL is significantly better in the RAI group based on these three domains since the mean scores were lower compared to the ATD group scores (goiter symptoms, 23.89 vs 32.17; emotional susceptibility, 44.82 vs 57.77; and impaired daily life, 29.46 vs 36.70). The remaining domains were found to be insignificantly different between groups despite lower mean final rescaled scores in the RAI group than the ATD group (p>0.05)(Table 4).
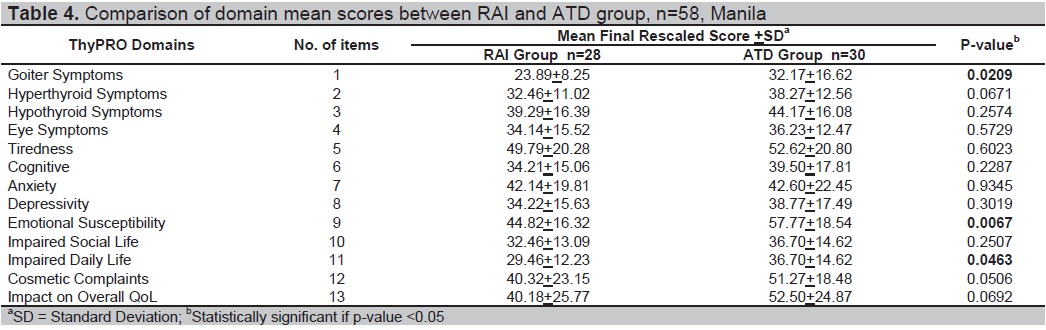
Table 4. Comparison of domain mean scores between RAI and ATD group, n=58, Manila
This means that goiter symptoms such as sensation or fullness in the neck, pressure in the throat and discomfort in swallowing are more common in the ATD group than RAI. For the emotional susceptibility domain, it showed that subjects belonging to the ATD group more easily felt stressed with mood swings as compared to the RAI group. In the impaired daily life domain, those in the RAI group have less difficulty in managing their life.
Correlation of Demographic Profile of the Participants with their Quality of LifeDemographic profile is correlated with their Quality of Life, as measured in the domains of ThyPRO Filipino version. Goiter grade was found to be moderately correlated with goiter symptoms (p=0.0001). Goiter grade is higher for those who did not undergo RAI with goiter symptoms such as sensation of fullness in the neck, pressure in throat and discomfort in swallowing. This means that the larger the goiter, the more is the neck discomfort. The domain “impaired daily life” and gender were weakly correlated (p=0.016) (Table 5). Female subjects scored significantly lower on the “impaired daily life” domain. This means that female subjects have lesser difficulty in managing their life, participate more in life activities and do not feel as if everything takes longer to do.
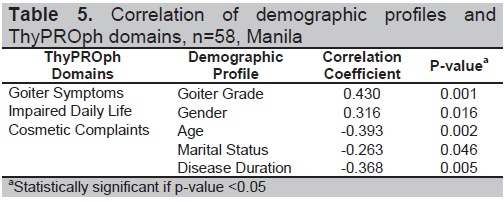
Table 5. Correlation of demographic profiles and ThyPROph domains, n=58, Manila
The domain “cosmetic complaint” was inversely and weakly correlated with age (p=0.002), marital status (p=0.046), and disease duration (p=0.005). Cosmetic complaints were higher among single young individuals with shorter disease duration.
First Phase: Translation and Validation
All the 13 domains were retained in the ThyPROph based on the statistics which showed that ThyPROph is an acceptable tool with Cronbach’s alpha and discriminant validity of 0.839 and 0.028-0.606, respectively and with moderate correlation for the convergent validity.
The translated and validated ThyPRO Filipino version (ThyPROph) can be used to assess the health related quality of life of adult Filipinos with Graves’ disease.
Second Phase of the Study: Comparison of quality of life scores with RAI treatment versus ATD Demographic Profile of Respondents and Health Related Quality of Life of Filipino Patients with Graves’ DiseaseIn this study, there are more singles in RAI group. In terms of fertility, it is a myth that RAI therapy for hyperthyroidism causes infertility. The exposure of the reproductive system to the dose of radioactive iodine for treating hyperthyroidism is just like when one is subjected for barium enema or intravenous pyelography. Uptake for the RAI in this case is concentrated in the thyroid gland.[14] The effect of RAI in male germinal epithelium is dependent on the cumulative dose. The risk of infertility contributed by hyperthyroidism per se is higher than the RAI itself.[15] A dose of up to 30 mci is harmless to the gonads.[16] In our country, the maximum fixed dose given as outpatient for Graves’ disease treatment is 14.9 mci.
Quality of life seems to be better in the RAI group compared to the ATD group with significant differences shown in the following three domains: goiter symptoms, emotional susceptibility and impaired daily life.
The RAI group was evaluated 7.76 + 8.77 years after initiation of treatment. At the time of interview for this study, patients belonging to the RAI group had reduced goiter size secondary to ablation and in their euthyroid state. RAI causes permanent destruction of thyroid tissue. The radioactive iodine after its uptake by the thyroid gland undergoes organification. Beta particles emitted damages the DNA and causes cellular necrosis destroying the thyroid follicular cells.[17] Reduction of thyroid volume is 30-40% after the first year and 50-60% after 3 to 5 years.[18] This is affirmed by the demographics in this study wherein the RAI group showed a trend of lower goiter grade. Lower goiter grade means lesser compression symptoms including fullness in the neck, pressure in the throat and discomfort in swallowing.
On the other hand, the ATD group evaluated 3.28 + 3.40 years after ATD initiation was euthyroid at the time of interview. ATD normalizes serum thyroid hormone levels 6 weeks after initiation. Relapse rate is highest with ATD at 50% when this is withdrawn. Demographics in this study showed a higher goiter grade in the ATD group. ATD preserves the thyroid gland with no reduction in size even after years of treatment since ATD only inhibits thyroid hormone synthesis. Large goiter is associated with lower remission rate.[19] Large goiters results to more compression symptoms impairing quality of life. In addition, remission is measured by TSH receptor antibody (TRab) levels. The higher the TRab level, the higher the rate of non-remission. In this study, the TRab level was not determined. Some of the patients belonging to this group although with normal FT4/TSH may not be totally euthyroid (not in remission) hence are more emotionally susceptible with impaired daily life quality.
Correlation of Demographic Profile of the Participants with Quality of LifeCompared to males, females use coping mechanisms by altering emotional responses to any stressful events.[20] This might explain the inverse relationship of gender and impaired daily life domain. These emotional responses can be positive reactions to the daily stressful events and to their Graves’ disease. In this modern world, cosmetic concern is the same in both genders and this study has shown as well that even single young men were concerned about their appearance.[21]
In conclusion, in this pilot study, despite both groups being euthyroid at the time of the survey, those who had undergone RAI had a better quality of life over-all and in the following domains: goiter symptoms, emotional susceptibility and impaired daily life. Nevertheless RAI can be considered as the better treatment option in our setting especially for patients who have noticeable goiters with symptoms attributable to their goiters, and those with emotional instability.
Limitations of the StudyAt the time of writing, there is no available data on quality of life of patients with Graves’ disease in our country. This pilot study intends to know if difference exists between two modalities of treatment by comparison of the quality of life. First limitation is the need for a larger scale study. A follow through large scale study will aid in making a generalization since the results of this pilot study is not powered to achieve the primary objective specifically in excluded patients with complications of Graves’ disease (e.g., thyrotoxic heart disease, hypokalemic periodic paralysis). Moreover, this study provides a brief account of the modalities used to treat Graves’ hyperthyroidism, specifically the use of anti-thyroid drugs and radioiodine ablation. Second, the reliability of the domains is reduced, despite the suitable overall reliability. The decision of the review committee to continue the use of the developed tool is on the assumption of the demographic readiness of the patients as a factor affecting the reliability of the tool. Demographic profiles (education, gender, age, occupation among others) of the subjects can influence response to translated tool. Thus, the committee’s decision on the use of the tool is based on the overall reliability of the translated tool. Third, a prospective randomized study is more ideal. All three were not carried out due to time constraint. Again, follow through study is recommended to generate satisfactory results.
AcknowledgmentsThis research work was completed with the help of ThyPRO questionnaire developer, Dr. Torquil Watt, Dr. Maria Honolina S. Gomez and the rest of USTH-endocrinology consultants and fellows, clinic secretaries of USTH consultants, and C.R. for analysis and interpretation of the data.
Statement of AuthorshipAll authors certified fulfillment of ICMJE authorship criteria.
Author DisclosureThe authors declared no conflict of interest.
Funding SourceNone.
[1] Melmed S, Polonsky KS, Larsen PR, Kronenberget. William’s Endocrinology, 13th ed. Philadelphia: Elsevier, 2016.