Graves’ ophthalmopathy (GO) is the most common extrathyroidal manifestation of Graves’ disease (GD).[1] It is the most frequent orbital disorder and is the most common cause of unilateral and bilateral proptosis in adults.[2],[3],[4] Internationally, it is detectable in approximately 10 to 60% of GD patients.[5] The prevalence of GO in Asians with hyperthyroidism was noted to be between 35% to 60%.[6]-[7] Locally, prevalence of GO was 48%, occurring more frequently among patients aged between 30 and 49 years. The most common signs were eyelid retraction, proptosis, and lid lag.[2] Unpublished reports show that GO comprised 24% of ophthalmology consults and was the leading cause of initial consult at the Orbit Clinic of the University of the Philippines-Philippine General Hospital (UP-PGH) in 2013 (unpublished data).
The major clinical risk factor for developing thyroid eye disease is smoking.[1],[8] Smokers are estimated to represent 64% of patients with GD and GO.[9] The risk of GO is found to be related to active smoking and is proportional to the number of cigarettes smoked per day. Previous smokers were also found to have significantly lower risk than current smokers.[10]
Other risk factors previously studied included genetic polymorphisms of the thyrotropin receptor. At present, genetic testing is not yet warranted as none of the polymorphisms impart a high enough risk of GO.[10] Thyrotropin receptor antibody (TRAb) may be useful in predicting course of GD and response to therapy but it is unknown if they are predictive of GO development.[10]
Iodine-replete areas show an increased incidence of autoimmune thyroid disease but its association with the development and progression of GO in Western countries has not been shown.[11] The Philippines is now considered an iodine-sufficient area based on a median urinary iodine level of 133 µg/L.[12] Iodine status showed no relation to the occurrence or progression of GO in a Danish population,[11] however, there are still no Philippine data at the moment.
Other risk factors related to autoimmunity are menarche at an age less than 15 years and late menopause (≥51 years of age) and is attributed to the estradiol effect. The use of oral contraceptives is said to have a protective effect against the development of GD due to yet unknown mechanisms.[13] A history of allergy is related to a slower decrease in TSH receptor antibodies, a lower chance of GD remission, and increased relapse owing to elevated levels of IgE.[13] Only an association with GD was elucidated in these studies but not with the development of GO.
The clinical presentation may vary from very mild disease such as tearing, photophobia, and conjunctival injection to severe irreversible sight-threatening complications due to compressive optic neuropathy.[3],[14]-[15] Overall, 13% of patients without GO at baseline will develop the condition. Of these, 42% will have mild GO and 2.6% will develop moderate-severe GO over an 18-month period during treatment with anti-thyroid drugs. For those with mild GO, 58% will show spontaneous improvement over an 18-month period, while about 2.4% will have progression to moderate-severe GO.[16] Approximately 6% of patients with GO develop optic neuropathy, a potentially blinding complication.[17] After an acute inflammatory phase lasting months, the chronic phase follows, characterized by hypertrophy and fibrosis of extraocular muscles, lacrimal glands and orbital fat, with subcutaneous eyelid changes which are permanent and unresponsive to immunosuppressive treatment.[14]
Management of GO is based on three pillars: restoration and maintenance of euthyroidism, smoking cessation, and rehabilitative surgery if warranted.[18]-[19] It can vary from watchful waiting and symptomatic management of eye dryness in mild disease to use of corticosteroids, radiotherapy and surgery depending on the severity of the condition.[19] Glucocorticoid therapy for GO has shown favorable response in 50 to 80% of cases, depending on route of administration but is not without adverse events.[20] Trials on efficacy of orbital radiotherapy report conflicting results,[19] and the procedure is associated with transient exacerbation of eye symptoms and risk of carcinogenesis, especially in younger patients. Orbital decompression as a form of rehabilitative surgery was associated with a 53% development of diplopia post-operatively.[21]
Compared to Caucasians, Asians in particular have earlier compressive features, increased orbital volume and a narrow orbital apex.[17] This finding further strengthens the need to promote early identification of patients likely to have progression of the disease. In the Philippines, studies on associated risk factors and predictors of severity as well as on long term outcome of this group of patients are still lacking. Despite advances in treatment, there are still no effective means of preventing GO or reliably altering its course. Current therapeutic options are aimed at the consequences of the disease rather than the cause. Unfortunately, these treatments do not prevent or reverse the pathological changes in the orbital tissues.[3] Apart from the medical implications of GO, data indicate that 45% of patients suffering from GO complained of restrictions in daily activities attributed to visual complaints with 38% reporting impaired self-perception.[22]
The lack of effective means of preventing or reversing GO and the variable effectiveness of available therapeutic options has shifted the focus on early detection and identification of patients most likely to have worsening of the condition.
This study aimed to describe the clinical profile of GD patients with GO, classify them based on activity and severity, and to determine the risk factors associated with the activity and severity of GO among patients at the UP-PGH.
METHODOLOGYThis was a cross-sectional analytical study done on 163 patients recruited from the outpatient clinics of Internal Medicine, Ophthalmology, Otolaryngology, and Family Medicine at the UP-PGH, a tertiary hospital in Manila, Philippines. Patients included were adults age 19 and above who were diagnosed with GD and have consented to participate in the study. Those who have other causes of thyroid-associated orbitopathy, such as those seen in Hashimoto’s thyroiditis and thyroid carcinoma, were excluded. Those who had undergone radioactive iodine therapy (RAI) or thyroidectomy as definitive treatment for hyperthyroidism were excluded, as well as those with a negative TRAb coupled with a low uptake on thyroid scan.
Using NCSS-PASS (Power Analysis and Sample Size) 2008 software, the minimum sample size requirement was at least 105 based on the percent of patients with severe GO among smokers and nonsmokers (0.33 and 0.107, respectively, with alpha level = 5% and power = 80%). Adjusting for a 20% non-response rate, the minimum sample size requirement was set at 132. Except for the alpha and power levels which were set by the researchers, all other parameters were taken from the study by Lee et al.[15]
All cases diagnosed with Graves’ disease at the outpatient clinics were screened. If found to be eligible, the participant was included in the study after giving consent. Complete history and physical examination was done by the principal investigator. A diagnosis of GD was made in the presence of hyperthyroid symptoms, laboratory evidence of elevated free thyroxine (FT4) and suppressed thyroid stimulating hormone (TSH), diffuse thyromegaly on ultrasound, and presence of TRAb. In the absence of TRAb, an increased uptake on thyroid scan confirmed the diagnosis.
The following data were collected from each patient: age in years, sex, history of thyroid storm, presence of comorbidities (such as diabetes, hypertension and other autoimmune disorders), history of atopy, current glucocorticoid use, family history of thyroid disease, duration of GD, antithyroid drug (ATD) used, duration of ATD treatment, and current FT4 level. A FT4 level greater than 24 pmol/L was considered to be elevated. For females, the following information were also obtained: age of menarche, late menopause (with late menopause being defined as cessation of menses > 51 years of age), and current oral contraceptive (OCP) use. Socioeconomic status was measured by monthly household income. High income class were defined as those households earning greater than PhP 2,393,125 (USD 47,537) annually or PhP 199,927 (USD 3,971) per month. Low income class were those with an annual income less than PhP 294,296 (USD 5,846) or PhP 24,524 (USD 487) per month. Those with an annual income falling between these amounts were classified as middle income households based on cluster analysis of population data and Consumer Price Index by the National Statistical Coordination Board.[23] Smoking history was reported as those who never smoked, previous smoker (defined as cessation of smoking before the diagnosis of GD) and current smokers.
All participants were then assessed at the Orbit Clinic for a complete ophthalmologic evaluation to determine presence or absence of GO. A board-certified ophthalmologist who was undergoing subspecialty training in Orbit performed the examination. Using the criteria of the American Academy of Ophthalmology guidelines,[2] GO was diagnosed if eyelid retraction occurs together with objective evidence of thyroid dysfunction, or exophthalmos, or optic-nerve dysfunction, or extraocular-muscle involvement. If eyelid retraction is absent, then GO may be diagnosed only if exophthalmos, optic nerve involvement, or restrictive extraocular myopathy coexists with thyroid dysfunction and no other causes for the ophthalmologic features are apparent.
Disease activity was assessed based on the Modified Clinical Activity Score (CAS) of the European Group on Graves’ Orbitopathy (EUGOGO)19 as described by Mourits et al., using clinical features of inflammation. The CAS will be based on the presence of each clinical feature for every patient. One point will be given for every criteria present: spontaneous retrobulbar pain, gaze-evoked orbital pain, eyelid swelling, eyelid erythema, conjunctival swelling or edema, conjunctival redness, and inflammation of the caruncle or plica. A CAS ≥3/7 indicates active GO. Patients found to have active GO were managed accordingly.
Disease severity was based on the classification of EUGOGO[19] with modifications used at the Orbit Clinic of the Philippine General Hospital. Severity was classified as mild, moderate to severe, or sight-threatening based on one or more of the following: lid retraction, soft tissue involvement, degree of proptosis, presence of diplopia, corneal exposure, and optic nerve involvement. Lid retraction was measured based on the distance of the upper or lower lid margins to the corneal light reflex, otherwise known as margin reflex distance (MRD). Measurement was done using a single millimeter ruler. Soft tissue involvement was determined based on the presence of periorbital swelling. The degree of proptosis was measured using a Hertel exophthalmometer. The normal value for Filipinos is between 10 to 19.5 mm. Proptosis was present if the measurement exceeded 19.5 mm, or if there was a difference of 3 or more between the two eyes. The presence of relative afferent pupillary defect (RAPD) pointed to optic nerve involvement.
A patient was diagnosed to have mild GO if any of the following were present: the MRD is less than 2 mm or if the upper lid retraction measures 4 or 5 mm, mild soft tissue involvement, degree of proptosis is less than 3 mm above the normal limit for Filipinos, no or transient diplopia, if corneal exposure is responsive to lubricants, and there is absent RAPD. A patient was diagnosed to have moderate-to-severe GO if any of the following are present: MRD >2 mm or upper lid >5 mm, presence of festooning or overhang of tissue, degree of proptosis is >3 mm above the normal limit for Filipinos, inconstant or constant diplopia, and negative RAPD. A patient was diagnosed to have sight-threatening GO if there is corneal breakdown and/or optic nerve involvement.
After ophthalmic evaluation, TRAb determination was done using a commercial receptor assay utilizing I125-labelled TSH (Immunotech s.r.o-Radiova 1, Prague, Czech Republic). Normal level is <1.0 U/L. Values between 1.1 to 1.5 U/L are considered equivocal. Values greater than 1.5 U/L were considered positive. Those found to have negative or equivocal TRAb titers underwent thyroid scan to determine uptake. A spot urine specimen was then collected for urinary iodine excretion (UIE) to determine iodine nutrition in this population. The urine specimens were sent to the Food and Nutrition Research Institute for processing using ammonium persulfate digestion with spectrophotometric detection of the Sandell-Koltholff reaction. A median UIE between 100 to 199 mcg/L is considered reflective of adequate iodine nutrition for the population. All specimens were stored and discarded using standard laboratory procedures.
This study underwent technical and ethical review by the hospital ethics board. Patient anonymity and confidentiality were maintained throughout the study.
Data AnalysisData analysis was done using Stata SE version 13, and included both descriptive and inferential statistics. Categorical variables were reported as frequencies and percentages. Continuous variables were reported as means and standard deviation if normally distributed, or median and interquartile ranges if not normally distributed. Comparison of characteristics between patients with and without activity was analyzed using independent t-test for quantitative variables, and Fisher’s exact test for qualitative variables. The association of the different factors with the activity and severity of GO was analyzed using logistic regression. The level of significance was set at 5%.
A total of 199 patients were recruited in this study. Five were excluded as they had undergone RAI before data gathering was completed. Thirty-one patients did not undergo ophthalmologic exam or had no TRAb or thyroid scan. A total of 163 patients were included in the analysis. The population came from low-income households and was predominantly composed of nonsmokers and females. The demographic and clinical characteristics of the study population are summarized in Table 1. The use of methimazole was comparable between those with active and inactive GO, as well as across GO severity groups. In our population, 127/163 (78%) had positive TRAb titers, with a median level of 8.9 U/L. Also, 52/163 (32%) had insufficient iodine intake with UIE levels of less than 100 mcg/L. 67/163 (41%) exhibited excess iodine intake with UIE levels greater than 199 mcg/L. Only 13/199 (8%) had active GO as the median duration of disease for this population was 2 years. The greater majority had mild disease (139/163 or 85%) while 8% had moderate to severe GO. Only 1 patient had sight-threatening GO due to the presence of corneal ulcers. None of the patients presented with optic neuropathy.
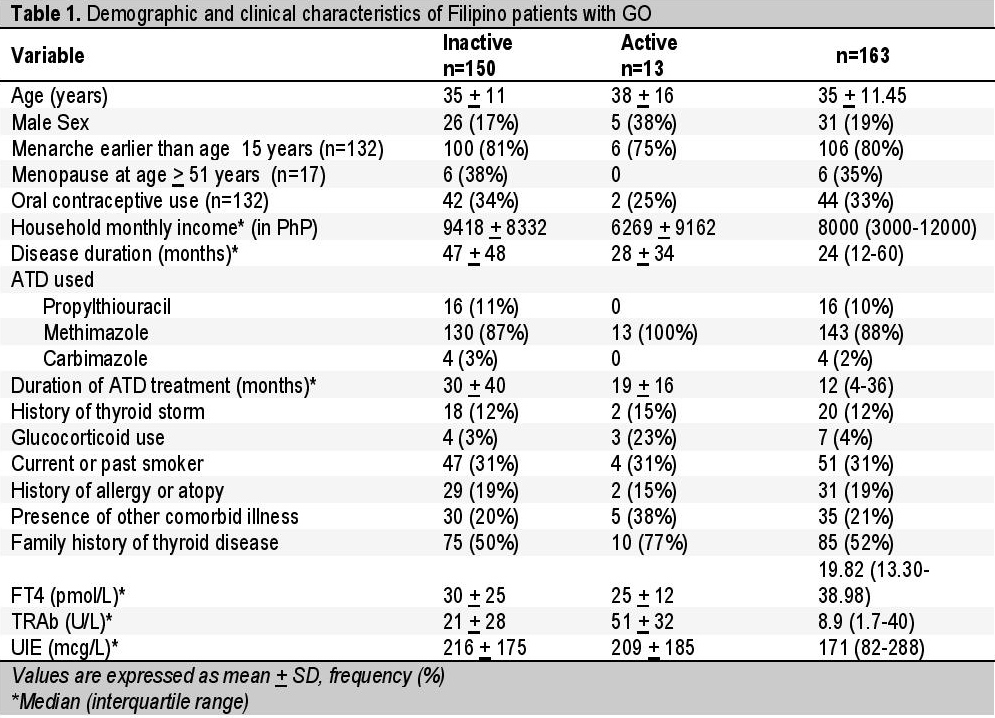
Table 1. Demographic and clinical characteristics of Filipino patients with GO
Patients with active GO tended to have had glucocorticoid use (p=0.012) and elevated TRAb titers (p=0.003). On univariate analysis (Table 2), elevated TRAb titers were found to be significantly associated with active GO. Smoking history, UIE levels, male sex, or duration of the disease were not significantly associated with active GO. Multivariate analysis of all significant factors revealed TRAb titers (OR 1.03, 95% CI 1.01-1.04, p=0.002) to be associated with active GO.
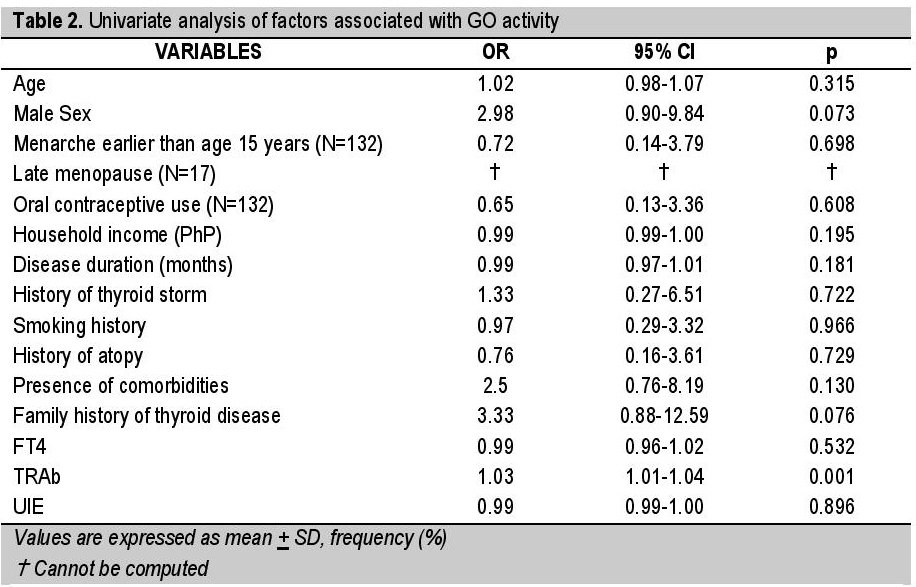
Table 2. Univariate analysis of factors associated with GO activity
Of the male participants, 5/31 (16%) had severe GO compared to 9/132 (7%) of female patients. Those with severe GO tended to have elevated TRAb titers (Mean 43 + 27 U/L; p=0.0097) compared to those with mild disease (Mean 22 + 29 U/L). Females with mild disease (44/149 or 36%) were more likely to be on an OCP (p=0.029). None of those with moderate to severe disease were on glucocorticoids. None of the females with moderate to severe disease had late menopause. The household income, disease duration, smoking history, FT4 levels, UIE levels, and treatment duration were comparable across groups. Univariate analysis (Table 3) showed elevated TRAb titers to be associated with increased GO severity. Multivariate analysis (Table 4) showed elevated TRAb levels (p=0.007) and male sex (p=0.041) to be associated with more severe GO.
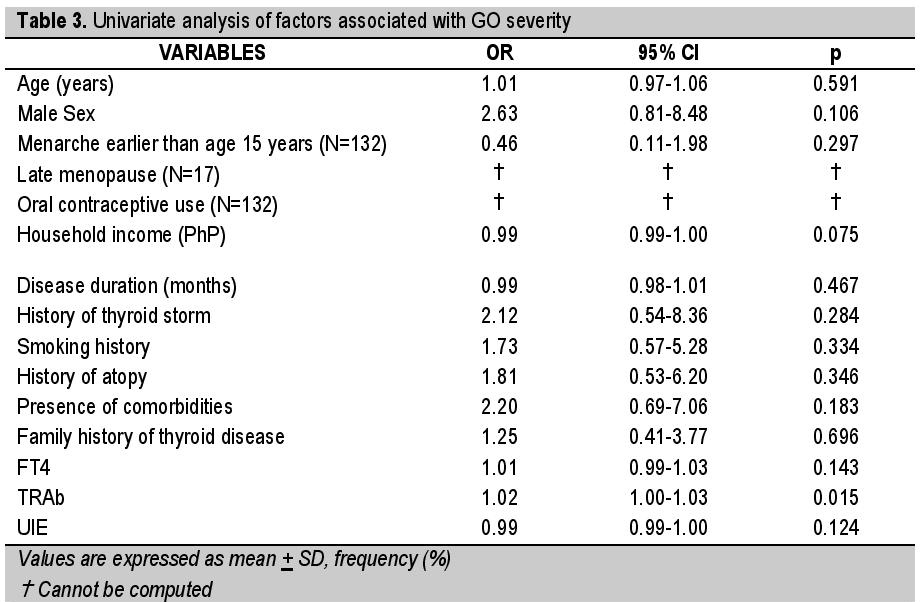
Table 3. Univariate analysis of factors associated with GO severity

Table 4. Multivariate analysis for GO severity
In this study we described the clinical characteristics of a younger, predominantly non-smoking Filipino population with GO seen in a tertiary university hospital in Manila who had GD for a median of 2 years and had been treated with anti-thyroid drugs for a median of 1 year. Only 8% exhibited active GO, likely as a consequence of having long-standing disease. The clinical course of GO, as characterized by Rundle,[24] is biphasic. Thus, the study population is mostly in the chronic fibrotic phase of GO wherein clinical indices of inflammation have already subsided. This is lower than the reported prevalence of active GO in the literature, which range from 11 to 32%.[25],[26],[27],[28] The differing rates of reported prevalence may be due to the use of varying criteria to define GO activity. Moreover, the duration of GD or GO was not reported for all studies. Thus it is unclear whether these were based on patients with newly diagnosed or longstanding disease.
The prevalence of moderate-to-severe or sight-threatening disease in our study was also lower than those reported in the literature,[6],[15],[25]-[26] with the exception of Tanda et al.,[16] who reported 5.8% of moderate-to-severe active GO in their newly diagnosed GD patients. As with the case of classifying GO activity, the criteria used to define GO severity were also dissimilar.
International data have shown several well-known risk factors associated with the development and deterioration of GO. These included (1) gender, with the disease being more prevalent in women but more severe in men, (2) smoking, especially smokers receiving radioactive iodine treatment, (3) radioactive iodine treatment, and (4) thyroid dysfunction including hyper- and hypothyroidism.[10]
Males have three times the risk of having more severe GO compared to females, corroborating previous reports. Surprisingly, smoking history did not show any significant association with both GO activity and severity. In contrast to other studies, our population exhibited a lower fraction of current or past smokers. The development of GO is associated more with the number of cigarettes smoked after the diagnosis of GD rather than the cumulative number smoked in a patient’s lifetime.[29] Previous studies have reported age to be associated with active[25] and severe GO, specifically dysthyroid optic neuropathy.[26] However, in our study, age was not associated with either GO activity or severity, similar to the report of Lee at al.[15] The duration of GD, duration of treatment with ATD, presence of comorbidities or atopy, family history of thyroid disease, UIE levels, and FT4 levels also did not show significant association with GO activity or severity.
Elevated TRAb titers emerged as a risk factor for both active and severe GO. Previous studies have reported conflicting results with regards to the association of TRAb with GO activity and severity.[15],[25]-[27],[30],[31],[32] However, these studies and our own differ in several respects: 1) duration of GO or GD in the study population; 2) criteria used to define activity; and severity, and 3) TRAb assay used. TRAb assays display wide intermethod variability,[33] thus contributing to the heterogeneity of results.
TRAb titers are expected to decrease following ATD therapy.[34] It is interesting to note that the titers for these patients are still elevated despite longstanding disease and ATD treatment. Given that majority of this population are already in the burnt out phase of GO, it seems that the autoimmune process is still ongoing despite the absence of clinical signs of orbital inflammation that is seen in active GO. Indeed, an observational study by Eckstein et al.,[35] reported that elevated TBII tiers at different time points after GO onset have higher risk of severe disease, independent of age and smoking.
The molecular pathogenesis of GO is still not precisely known. Orbital fibroblast have been shown to express functional thyrotropin receptors (TSHR), making them possible target cells. It is postulated that enhanced activation of the TSHR results in hyaluronic acid synthesis and adipogenesis in the orbit,[36] which are the pathologic hallmarks of GO. Whether TRAb is the one which effects this activation is not yet known with certainty. Another putative self-antigen postulated to underlie GO is insulin-like growth factor-1 receptor (IGF-1R). It is theorized that TSHR and IGF-1R are involved in the crosstalk to effect the pathologic changes in GO through any of the following mechanisms: 1) binding and activation of IGF-1R by stimulating IGF-1 like agonists; 2) enhancement/inhibition of TSHR signaling by IGF-1R; or 3) physical hybridization of a functional tyrosine kinase and G protein-coupled receptor.[37]
Given that the TSHR is postulated to participate in the pathogenesis of GO either as an autoantigen or as a molecular conduit for downstream signaling,[38] the demonstration of a clinical association of TRAb with GO activity and severity makes it a possible contributor in the pathogenesis of the disease.
However, our study is limited in several aspects. First, the population included patients in a variety of stages of GO, as evidenced by the wide range in disease duration. Second, only a small proportion exhibited active or severe GO. The sample size may not have been enough to elucidate the association of the variables with disease activity or severity given the low smoking rates and low prevalence of active or severe GO. Moreover, the cross-sectional design precluded determination of causality from the associations observed in this study. Lastly, the assay used cannot differentiate between stimulating, blocking, and neutral antibodies. There is a heterogeneity in the types and affinity of TRAb in a single patient.36 In order to confirm the association found in this study, future investigators should look into prospective or longitudinal studies on new-onset GO with repeated determinations of TRAb over the course of the disease, utilizing assays that can differentiate the different types of TRAb. This may help determine if TRAb will be clinically useful in prognosticating the course of GO for patients.
This study reported lower rates of active GO and moderate-to-severe or sight-threatening GO compared to those reported in literature. In this cohort of predominantly nonsmoking Filipinos with GO, an elevated TRAb titer emerged as a risk factor for active GO and a severe disease course.
AcknowledgmentThe authors recognize Erlinda Dacanay, RMT of the Radioimmunoassay laboratory of the Philippine General Hospital for performing the TRAb assay on all patients.
Statement of AuthorshipAll authors certified fulfillment of ICMJE authorship criteria.
Author DisclosureThe authors declared no conflict of interest.
Funding SourceThis study was a recipient of the Philippine Society of Endocrinology, Diabetes and Metabolism research grant in General Endocrinology.
[1] Abboud M, Arabi A, Salti I, Geara F. Outcome of thyroid associated ophthalmopathy treated by radiation therapy. Radiat Oncol. 2011;6:46-51. PubMed Central DOI.